Opinions
Biden administration must overhaul monkeypox response now
We need a plan emphasizing equity in vaccination, testing, treatment
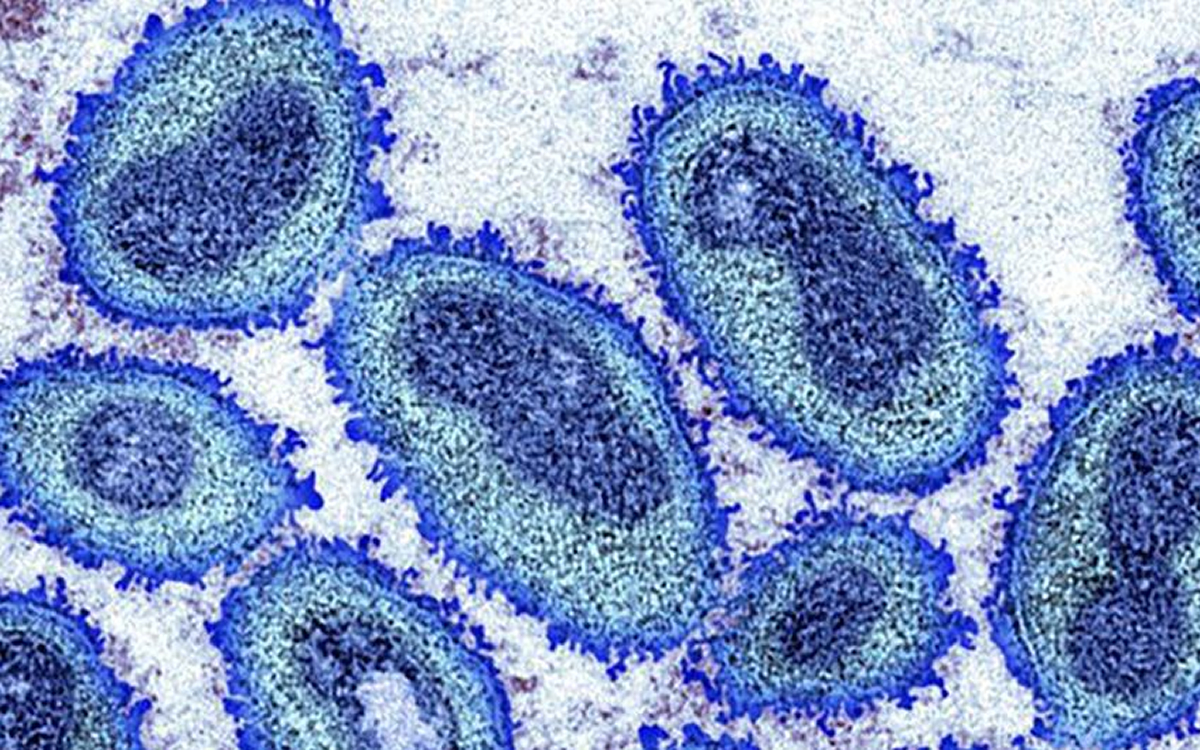
The Biden administration needs to overhaul its response to monkeypox. Now.
For many who were around during the height of the AIDS epidemic, the Biden administration’s missteps around monkeypox are pale but haunting reminders of past battles. That’s particularly galling for LGBTQ+ Americans as more than 95% of monkeypox cases in 2022 are striking men who have sex with men (MSM).
The Centers for Disease Control and Prevention (CDC) estimates 1.6 million Americans are at risk, requiring 3.2 million doses. But outreach has been ineffective. Not even 10% are fully vaccinated.
It’s imperative that the White House implement a comprehensive plan emphasizing equity in prevention, vaccination, testing, and treatment. In August, the administration irresponsibly decided to withhold monkeypox vaccines from Americans whose health agencies aren’t using a newly mandated injection method. Washington theorizes the more efficient intradermal (ID) method will quintuple doses from vials.
Health officials from D.C. to Seattle report averaging 3.5 doses per vial amid significant disruptions. The Association of State and Territorial Health Officials echoed their claims.
Using flawed assumptions that healthcare providers will extract five doses from each vial, the Biden administration is sending one-fifth of the vials previously allotted. That eliminates 100% of their imagined increase, but Washington is sending around 30% fewer usable doses compared to pre-mandate allotments. “The federal government has patted themselves on the back for how they’re accelerating the delivery of vaccines,” reflected DC Department of Health Senior Deputy Director Patrick Ashley. D.C. has nearly the highest case rate in the nation. “What they did is they moved numbers around.”
We urge President Biden to reinstate original vial allocations. The point of doing ID, noted Johns Hopkins scholar Caitlin Rivers, was to “benefit from the increase in supply.”
While we hope JYNNEOS’s two-shot course proves safe and effective, data is scant for subcutaneous use, and more so for ID – particularly for people who are immunocompromised, including those living with HIV. One study, reported STAT, showed one dose providing nearly undetectable protection. And some agencies still aren’t scheduling second injections. Even its manufacturer documented reservations about the administration’s approach.
Contends one writer in The Atlantic, “The FDA is now playing a high-stakes game with the health and trust of people most vulnerable to monkeypox…” It typically causes rash and flu-like symptoms, but lesions around the anus, genitals, or mouth are excruciating. An oft-cited study shows JYNNEOS’s efficacy, but it’s based on a 2010 trial of approximately only 175 mostly young, white, healthy straight men receiving ID.
The reduction in doses has forced some jurisdictions, like Philadelphia, to scale back vaccine outreach, complicating plans for required second doses. While cases are disproportionately high among Black and Hispanic individuals, vaccination among Black people remains exceedingly low. Reasons include distrust, stigma, and less accessible vaccine centers.
The White House has allocated 10,000 vials for local networks to vaccinate under-vaccinated demographics, especially people of color. It should be 100,000. Still needed: a detailed commitment to vaccinate incarcerated and un-housed individuals.
Up to 15% of Black and Hispanic individuals – populations most at risk of contracting monkeypox – and 5% in Asian communities are prone to keloid scarring, which causes skin discoloration. For those affected, ID would be ineffective and likely harmful, and damaging to trust of the public health community.
ID’s smaller doses are also deepening skepticism in vulnerable communities. The shrunken supply and over-emphasis on intradermal injections will exacerbate existing racial and socioeconomic disparities in vaccination. We must not allow this. Promoting the subcutaneous option is critical to encourage vaccination, especially for those ineligible for ID.
Demetre Daskalakis, White House Deputy Coordinator for monkeypox, anticipates “real-world” data from health agencies on “actual doses from vials.” After issuing the mandate?
Daskalakis and CDC Director Dr. Rochelle Walensky indicate jurisdictions can request more vials, including for subcutaneous injections, but their vagueness has prevented some agencies from scheduling second shots.
Monkeypox was confined to Africa, where health resources are poor. Out of our sight, it was out of mind — until 27 countries where it hadn’t existed reported 780 cases in May. The World Health Organization declared a public health emergency on July 23. President Biden didn’t until Aug. 4. Five weeks later, domestic cases had more than tripled to 21,274.
Biden has often said, “Help is on the way.” It’s taking the long route. In his first joint address to Congress, Biden told transgender Americans – who are at high risk of contracting monkeypox – “Your president’s got your back.” As we advocate for speedier, more equitable vaccination, that assurance could use its own booster.
Dennis Jaffe of D.C. is an active member of PrEP4All’s monkeypox advocacy project. He has 40 years of professional experience in grassroots advocacy for social justice causes.





Opinions
D.C. queer faith leaders commit to exist, resist, persist
Pride Interfaith Service features remembrances, celebration

Last month, Center Faith hosted the 43rd annual Pride Interfaith Service titled “In Faith We Exist. Resist. Persist!” at St. Mark’s Episcopal Church in Washington, D.C. Amid torrential downpours, queer leaders and people of faith from Muslim, Catholic, Episcopalisn, Unitarian Universalist, Jewish, Pagan, and many other communities gathered in a church immediately behind the John Adams building.
In the two-hour service, leaders spoke about the power of faith in the fight for LGBTQ rights and against Chrisitan nationalism, all while honoring three lifelong leaders in the D.C. LGBTQ interfaith community.
The service began with Rev. Michelle Morgan welcoming everyone to St. Mark’s Episocal Church, followed by greetings from Robert Sanchez, representing The DC LGBTQ+ Community Center, Japer Bowles, representing the D.C. Mayor’s Office of LGBTQ Affairs, and Danielle Goldstone, representing the Interfaith Council of Metro Washington.
Rev. Ebony Peace, a Unitarian Universalist community minister and one of the service organizers, welcomed everyone with a blessing:
“Today in this interfaith worship service, we celebrate our existence. We honor those past and present who resist oppression. We acknowledge today that the fight for freedom and dignity is not over. We will be here. We will not be silent, and we will not back down.”
Representatives from diverse faith traditions followed by creating and blessing the space with a libation ritual by Rev. Elder Dr. Akosua McCray from Unity Fellowship Church of Washington, DC, a recognition and grounding in the elements by David Dashifen Kees from The Firefly House, along with readings from Aura Kaiser (DC Queer Muslims), Daisaku Leslie (Sokka Gakkai International), and Jonah Richmond and Rachel Dubin from Jewish temples throughout the Washington, DC area.
Rev. Cathy Alexander and her partner Dr. Carla Sherrell shared an offering on love, an interpretation of 1 Corinthians 13 and a contemporary meditation by Rev. Tess Baumberger on behalf of the Metropolitan Community Church in DC, followed by words of joy by Rev. Thomas Wieczorek from the National Catholic Church and silent meditation led by Joe Izzo from the Friends Meeting of Washington.
After songs and responsorial affirmations, Bishop Mariann Budde, who is perhaps best known for delivering the homily at the January 2025 interfaith prayer service immediately following Donald Trump’s second presidential inauguration, spoke at the service. In her gentle but determined voice that reverberated throughout the space, she asserted that “I’m here tonight to affirm the unshakable goodness of each person here and of every person, and to say without equivocation that what needs to be resisted by each and everyone one of us is anything that would negate that goodness, that would cause any of us to feel less than worthy of love and belonging.”
She was followed by a beautiful call and response song led by Cantor Ze’evi Tovlev from Temple Shalom titled “The Birds Don’t Know.” As Cantor Tovlev sang the words “I will sing a song of mourning, I will transform and let go,” this service shifted to recognizing–as it had when Elder Akosua McCray led the libation ritual, all the queer and trans elders who have gone before us, including one of the honorees this evening: SaVanna Wanzer who passed away in April of this year.
SaVanna Wanzer was one of the original founders of DC Trans Pride and DC Black Trans Pride. As one of the first leaders creating transgender programming at DC Black Pride, she fought to represent and celebrate her lived experiences, and as a Black trans woman living with HIV, she regularly volunteered for DC’s Whiteman-Walker Health clinic and became the first recipient of its Robert Fenner Urquhart Award recognizing her service. What many people do not know is that Wanzer was an active member and ordained Deacon at Westminster Presbyterian Church, which hosted the first Transpride event in Washington, DC.
At this year’s service, she was honored by Rev. Danielle Dufoe, a Presbyterian minister who is the first Black trans woman to complete both divinity and seminary school, who called the fierce advocate and friend both “mother” and “champion.”
“We need folks like SaVanna, and we need folks like Jesus,” Dufoe said, “who says no man takes my life but I lay it down for the sake of salvation. And SaVanna is saying no man took my life. I laid it down for beloved community.”
Following a remembering of Wanzer’s life, Rev. Dr. Wallace Charles Smith recognized Bishop Cheeks, affectionately known as “Rainey,” is a native Washingtonian who founded Inner Light Ministries in Washington, DC in 1993. Before his time as an ordained minister, he was the lead coordinator for the famous DC “Clubhouse,” where the LGBTQ+ community found both social and spiritual refuge in a space that was totally drug and alcohol free. Continuing the spirit of the “Clubhouse,” he founded Us Helping Us, an organization supporting African Americans who live with HIV/AIDS that fought shame and stigma inside and outside of the LGBTQ+ community.
“Through his ministry and public witness, countless individuals found the courage to live authentically and to claim both their faith and their identity. Tonight, as we affirm that in faith, we exist, resist, and persist, we celebrate a man who has done exactly that. He has existed unapologetically. He has resisted exclusion, stigma, and injustice. He has persisted through epidemics, discrimination, silence, and struggle,” Smith said.
“And through it all, he has continued to remind us of his enduring spiritual affirmation. I see the God in you,” Rev. Smith’s voice thundered as he turned to face his mentor and friend.
Finally, Rev. McCray, a Black lesbian founding pastor of Unity Fellowship Church of Washington, DC, recognized Michael Vanzant. Vanzant served as co-pastor of Faith Temple in Washington, which has described itself as the nation’s first explicitly Black, gay Christian congregation. Vanzant took over the reins after its founder–Dr. James S. Tinney–died in 1988 of AIDS. Although he stepped away from his role as co-pastor several years after succeeding Tinney, he assumed a pastoral role again in the early 2000s and has continued fighting for LGBTQ+ inclusion in Christian and interfaith spaces ever since, serving on the organizing committee for the Pride Interfaith Service.
McCray shared that “the power that he gave to people to preach, to sing, he gave them rope to pull people at the other end toward them.”
The two living honorees — Cheeks and Vanzant — were presented with certificates expressing the community’s gratitude.
A small celebration with food was held in the parish hall after the conclusion of the service that many described as “profound and moving.” Although fewer people than normal attended the service–approximately 60 people in total, it was an important moment for many queer and trans people who are navigating their relationship with faith, especially as far right actors use religion and religious liberty to justify their anti-LGBTQ+ policies.
Amid the rise of Christian nationalism asserting a heternormative, trans-exclusionary politic, faith leaders affirmed the power of queer and trans people to claim and become empowered by faith.
Emma Cieslik is a D.C.-based museum worker and public historian.
Opinions
Democratic Socialists of America are not automatically Democrats
There’s some overlap but also major policy differences

I recognize people come to their opinion of the Democratic Socialists of America Party, a party different from the Democratic Party, usually based on their own backgrounds.
I am a progressive Democrat. A first generation American; gay, and Jewish. My parents were refugees from Hitler, my mother from Austria, my father from Germany. My father’s parents were killed in Auschwitz. I have spent a lifetime working for civil rights, women’s rights, disability rights, and since I came out at the age of 34, LGBTQ rights. I was a union member when I taught school in Harlem. I worked for one of the most progressive members of Congress, Bella S. Abzug (D-N.Y.). Bella understood how to move forward the progressive issues she worked on. She won the right for women to get their own credit cards, without their husband’s signature. She is responsible for the curb cuts we see on every corner. She was the first to break the highway trust fund for mass transit. She fought against the Vietnam War, and to impeach Nixon. She introduced the first Equality Act for the LGBTQ community. She was named a whip by Tip O’Neill in her third term in Congress, not because she gave up her fight for progressive causes, but rather because she could get things done. She understood what compromise meant, and used it to move forward the progressive issues she fought for.
So, people must understand, members of the Democratic Socialists of America (DSA), are their own party, they are not automatically part of the Democratic Party. They have their own platform, different from the Democratic Party platform in many ways. Yes, the two overlap in many areas. But the differences are clear.
DSA was founded in 1982 from a merger of the Democratic Socialist Organizing Committee (DSOC), and the New American Movement (NAM). The merger was seen as a symbolic healing of the rift between the Old Left, represented by DSOC’s social democrats and trade unionists, and the New Left, represented by NAM’s activists who emerged from the social movements of the 1960s. Initially led by Michael Harrington, the DSA continued DSOC’s strategy of “realignment” by working within the Democratic Party to push it to the left, functioning as a small advocacy group for its first three decades. After the 2016 presidential campaign of Sen. Bernie Sanders, a self-identified democratic socialist, and independent, never a Democrat, and the election of Donald Trump, the organization’s membership swelled from about 6,000 members in 2015 to 100,000 in 2026. This growth gave DSA a much younger and more activist base, which shifted its strategy toward one centered on building an independent political force. DSA’s platform calls for reforms such as a Green New Deal, single-payer healthcare, and tuition-free higher education, with a long-term aim of social ownership and democratic control of the American economy. They support defunding the police. DSA’s foreign policy is non-interventionist, strongly supporting spending cuts and footprint reductions to the U.S. military while also supporting pro-Palestinian and anti-Zionist causes. That includes the abolishment of the State of Israel from the ‘river to the sea.’
As a progressive Democrat, I support universal healthcare, and have since Hillary Clinton introduced it to Congress when she was first lady in 1993. I support expanding Medicare, ensuring the solvency of the Social Security System, and making housing, childcare, and education, affordable for everyone. As a Democrat all my life, I supported Democrats who believe in the same things.
This may enrage many, but in my opinion one of the biggest mistakes the Democratic Party made was allowing independent, Democratic Socialist Bernie Sanders, to run in their presidential primary in 2016. When they did, they shared their voter lists, and enabled Sanders to get a foothold in the party without actually being a Democrat. He ended up screwing Hillary Clinton’s chances to be president. He attacked her throughout the entire primary, and even after she secured the nomination, he kept attacking, and wouldn’t endorse her for 30 days. When he finally did, he traveled the country, in essence pretending he was campaigning for her, when in actuality he was building his own brand, and writing his book. So yes, the independent, Democratic Socialist, Bernie Sanders, who has accomplished nothing in a 40-year congressional career, carries a lot of responsibility for helping to elect Donald Trump.
Today we have Mamdani, mayor of New York, who proudly calls himself a Democratic Socialist of America. He is a charismatic leader, and helped a number of Democratic Socialist candidates in New York win their primaries. One who he endorsed for the state Senate in Queens, is Democratic Socialist Aber Kawas. She is the one who said the United States brought the 9/11 terror attacks on itself, believing we asked for and are responsible for the nearly 3,000 people killed.
I have been, and will be, attacked, for saying the DSA platform is anti-Semitic for calling for the total abolishment of the State of Israel. For asking why there is nowhere in the DSA platform a condemnation of Hezbollah or Hamas, for their platforms calling for genocide against Jews in the State of Israel, while they are comfortable calling Israeli killings in Gaza genocide. While I may debate the term, I agree what Israel is doing is horrendous. Netanyahu and his government are committing war crimes, and belong in jail. But then so are Hamas, and Hezbollah committing war crimes.
The way to stop all this is to rid the world of Netanyahu and his government, and the terrorist groups Hamas and Hezbollah. I believe the United States should stop funding Israel’s offensive weapons, while we still ensure they have an adequate defense. Iran and others need to stop funding the two terrorist groups. We need to separate people’s views of the Jewish people, from the Netanyahu government, in the same way we need to separate views of the Palestinian people from Hamas, and the Lebanese people from Hezbollah. That is the only way we will ever have peace and a Palestinian state. If we ever get there, we must ensure the billions of dollars needed to make it self-supporting. But to get to that state, the Palestinian people must also have the support of the world, including the states surrounding Israel, that have never given support to the Palestinian people. I don’t have an answer to all of this, and clearly no one else does at the moment. I believe the last time there could have been a Palestinian state, with Israel agreeing to it, was back during the Camp David accords.
But whatever happens in the Middle East, if we want people in the United States to succeed, if we want to make sure the poor and the middle class can do more than just exist, if we want to provide affordable, decent healthcare, housing, job opportunities, and childcare, etc., the Democratic Party must not think redefining themselves as the Democratic Socialists of America, and all the baggage they bring with them, is the way to go.
While DSA candidates will succeed in a few big cities, this is not where the vast majority of voters in the nation are. If there is a positive Democratic Party platform, and we allow candidates in each district to run on the particular issues they feel can win for them, we can move the vast majority of the nation to more progressive positions, and to younger Democrats. That is the direction the Democratic Party must move in if we are to take back Congress in the midterms, and then the presidency in 2028.
There are a host of candidates around the country who are running, and winning, in Democratic primaries, as Democrats, not as members of the DSA Party. In not one of the districts we need to flip to take back Congress, is being a member of the Democratic Socialists of America a positive thing.
To begin the process of taking back our country, let’s all support Democrats across the board, up and down the ballot. If we do, we win!
Peter Rosenstein is a longtime LGBTQ rights and Democratic Party activist.
Opinions
Actually, I’m gay and I’m queer. It matters
Matthew Vines in New York Times argues ‘queer’ identity prompting anti-LGBTQ backlash

Yesterday, on the last day of Pride month, the New York Times published an opinion piece by Matthew Vines where he argued that the push to identify as “queer” is a contributing factor to modern backlash to LGBTQ+ rights. In the piece, he argues that “being gay is not a rebellion against ordinary life.” As a queer public historian, I disagree — being LGBTQ+ is a revolutionary act because American society was and continues to be built on heternormative, cisgendered standards. We need only look at yesterday’s Supreme Court decision upholding bans on trans athletes to realize that LGBTQ+ rights are still greatly under attack.
Vines and other white cis gay men and women who refuse to use the term “queer” or understand their bodies, identities, and relationships as political fail to recognize what secured their rights protecting them against discrimination and to marry the people they love.
Remember your ancestors
The Stonewall riots, largely considered the birth of the modern LGBTQ+ movement, was a reaction against a police raid that began in June 1969. It was groundbreaking pushback against systemic police brutality and state-sanctioned incarceration of and violence against LGBTQ+ people, and by and large, these riots — which mobilized the larger LGBTQ+ community — is the reason that lesbian, gay, and bisexual people have the right to marry the people they love.
It is because of Black queer and trans people — people who recognized that queerness is a political act as much as it is an identity — that Vines’s rights were secured in the first place. Denying the identity of “queer” not only perpetuates the very stigma surrounding this word but that which surrounds queer and trans people as a whole, and it denies the rich legacy of our queer and trans ancestors who fought for the rights we have today. When queer and trans people reclaimed the word “queer,” previously a slur against us, it was a call to resist the very gender and sexual assimilation that made the weaponized the slur itself.
Because at its very core, the United States remains a nation that enforces and exalts a heterosexual, cisgender majority. To be queer, to resist and reject standards that normalizes and essentialize gender and sexuality, is a countercultural act, whether or not people like Vines are ready to acknowledge it. Historically, there has been a contingent of the LGBTQ+ community, largely those with the most privilege, who have historically and presently attempted to sanitize the community’s image and its events — to exclude trans people, kink and BDSM, and drag — on the grounds that they infringe on a family-style event and “give the community a bad name.”
Freaks Are family
Back in 2000 the Millennium March on Washington pushed for gay and lesbian assimilation, arguing that they — we — are like everyone else. Vines appears to copy and paste this language into the piece he published yesterday. But in response, the “Freaks Are Family Contingent,” a group organized by the DC Radical Fairies and Bi Insurgence, marched as an alternative to the main group. This group, which purposefully included witches, trans people, people practicing kink, and people who are poly, called out assimilation as perpetuating the same marginalization that gay and lesbian people faced 50 years ago. To this day, “Freaks Are Family” remains a rallying cry for radical inclusion and resisting assimilation in Washington, D.C., and beyond. One of my dear friends — Rev. Eric Eldritch, a long-time Radical Faerie and community leader in Washington, D.C. — was part of this groundbreaking movement.
Maybe Vines has a point. There are members of the LGBTQ+ community that remain settled and complacent in their privilege and refuse to recognize the fragility of their and others’ civil liberties. As historians and political scholars have argued, attacks on trans people’s rights will likely proceed threats against same-sex marriage, which itself was secured just over 10 years ago.
Risking his and our rights
On the 10th anniversary of Obergefell v. Hodges, Oklahoma senator Dusty Deevers said that gay marriage is not law because “there is just no right ot gay marriage in the constitution.” Deevers made this comment during a conversation with Tony Perkins, president of the Family Research Council, who believes that the Bible justifies Christians killing gay people. The news was first flagged yesterday by Right Wing Watch, a watchdog group for far-right action, and further by LGBTQ Nation voicing concern for his inflammatory statements about drag queens and LGBTQ+ books in elementary and middle schools.
Deevers clarified that “Obergefell isn’t settled law. It’s besetting immorality imposed by judicial decree, and court opinions can be referred to as ‘settled law’ only if they are rooted firmly in the Constitution and the heritage and the tradition of the American people.” This is pointedly incorrect, but it is an argument that is increasingly being used by far-right leaders to argue that precedent-setting decisions are not set in stone.
What largely kicked off this moment was the Supreme Court overturning Roe v. Wade in June 2022. The pivotal ruling handed down in 1973 ensured federal access to reproductive justice, and yet nearly 50 years later, it was overturned and followed by a number of states instituting their own laws banning abortion, even in situations of life and death. People have died not only because of these bans but because of medical professionals’ hesitancy to provide vital, lifesaving care for fear of losing their medical licenses or being sued.
Thus, it made sense to many LGBTQ+ activists in 2022, that same-sex marriage legal protections, especially those from the landmark 2015 Supreme Court Case Obergefell v. Hodges would be the next to fall.
Right after the U.S. overturned Roe v. Wade in 2022, Justice Clarence Thomas released an opinion stating that the court should also reconsider the decisions in other landmark cases, such as Griswold v. Connecticut, Lawrence v. Texas, and Obergefell v. Hodges. These rulings protect access to contraception, LGBTQ+ relationships and marriage. And like Deevers’s call today, Lawrence also argued three years ago that the Due Process Clause in the Constitution does not secure any of these rights. Calls to overturn Obergefell v. Hodges is rising day by day, and distancing himself from queer people and the wider movement will not protect him.
In truth, Vines’s opinion piece reveals that he is pointedly not “queer,” but as many queer people have called out in the last 24 hours, that is not a good thing. When he and others fail to be not only support but participate in the revolutionary movement to liberate all LGBTQ+ people, to stand and fight in solidarity with trans, nonbinary and intersex people who are repeatedly targeted by the government, stripped of their identification documents and access to public spaces, and killed for who they are, they are part of the problem.
They become the very marginalizers that 50 years ago targeted people like them — the white cis gay men and women — who lost their jobs and their lives for who they loved. Truly Vines is not “queer,” but in doing so, he not only compromises the strength of the very community that secured his present rights to live and love authentically but the rights to do so in the future.

Under-the-radar Delaware beach towns smart buyers are targeting

‘My Favorite Sociopath’ debuts at Shepherdstown’s CATF
‘Transcendent’ a tough but important read

SMYAL receives $25,000 award for ‘courageous acts’

Queen Camilla meets with JK Rowling

Gay US couple among four people found dead in Mexico mass grave

ACLU says trans athletes ruling is narrower than many believe

Centenares de personas participan en la Marcha del Orgullo en la capital salvadoreña

Delaware approves amendment protecting same-sex marriage

Actually, I’m gay and I’m queer. It matters
-

 Mexico5 days ago
Mexico5 days agoGay US couple among four people found dead in Mexico mass grave
-
National5 days ago
ACLU says trans athletes ruling is narrower than many believe
-
Noticias en Español5 days ago
Centenares de personas participan en la Marcha del Orgullo en la capital salvadoreña
-
Delaware5 days ago
Delaware approves amendment protecting same-sex marriage



