National
What’s next for health care reform?
After court ruling, focus turns to state plans for Medicaid

Now that the Supreme Court has upheld the constitutionality of President Obama’s health care reform law, advocates are pushing for additional efforts to extend coverage of the law to LGBT people and people with HIV/AIDS to the fullest extent possible.
For the most part, the next step in the process involves looking to the states to determine whether they will adopt health policies afforded to them under the law — foremost among them is the Medicaid expansion to cover all people with incomes up to 133 percent of the federal poverty level.
Although the Supreme Court ruled the majority of the health care law is constitutional, it prevented the federal government from withholding all Medicaid funds from states if they decline to take part in the Medicaid expansion. As a result, states can decide whether or not to enter the expansion without fear of losing money.
Patrick Paschall, a policy advocate at the National Gay & Lesbian Task Force, said the Medicaid expansion is particularly important for LGBT people because they disproportionately live below the poverty level.
“The Medicaid expansions are going to end up being hugely important for LGBT people because it expands coverage to low-income people, and LGBT people are disproportionately low-income,” Paschall said. “We know this because of rampant employment discrimination and housing discrimination.”
A report on transgender people published earlier this year by the Task Force and the National Center for Transgender Equality, titled “Injustice at Every Turn: A Report of the National Transgender Discrimination Survey,” found that transgender people experience unemployment at rates twice that of the national population, and black transgender people experience it at a rate of four times as much.
Carl Schmid, deputy executive director of the AIDS Institute, said the Medicaid expansion is particularly important for people with HIV/AIDS because of 50 percent of those in care rely on that program for support and those numbers will “grow substantially” if states decide to participate.
“Those who are really poor, they’re going to be covered under Medicaid,” Schmid said. “The question is what are we expecting from the states.”
But a number of states may not take part. According to a report in The Hill newspaper, at least 15 governors have signaled they won’t participate in the Medicaid expansion now that the Supreme Court has enabled them to wiggle out of participation.
Florida Gov. Rick Scott, a Republican elected to office during the Tea Party wave in 2010, was among those saying his state wouldn’t take part in the Medicaid expansion — or other parts of the health care law that are optional to the states.
“We’re not going to implement Obamacare in Florida,” Scott said last week on Fox News. “We’re not going to expand Medicaid because we’re going to do the right thing. We’re not going to do the exchange.”
Under the health care reform law, the federal government will pay for the Medicaid expansion for the first few years. Expenses for states come up in 2017, when the federal government will pay 95 percent; That’s reduced to 94 percent in 2018 and in 2019 it goes down to 93 percent. Starting in 2010 and then on out, the federal government will pay 90 percent of the total amount.
Schmid said the bargain that was set up for states under the health care law makes the governors’ decision not to participate in the law questionable.
“Here their taxpayers are going to be paying their taxes to pay for this; this is federal funds,” Schmid said. “Their state is not going to take responsibility for covering. The hospitals? Don’t they want people to be covered? They’re going to have unconstituted care if they don’t.”
For the states that don’t participate in the Medicaid expansion, Schmid said people living there with HIV/AIDS will have to continue relying on the Ryan White Care Program, which provides funds for AIDS medications for low-income people with HIV. The program will be up for reauthorization in 2013.
As advocates push for states to adopt the Medicaid expansion, the law has several key components that already offer protections and benefits for LGBT people and people with HIV/AIDS. State and federal health insurance will be set up in the law starting in 2014.
For the first time, the law extends federal non-discrimination protection in the health care system on the basis of gender.
Paschall noted that provision is key as courts and agencies have determined that discrimination against transgender people amounts to gender discrimination.
“We know that federal agencies like the Equal Employment Opportunity Commission, the Department of Housing & Urban Development as well as federal courts have interpreted sex-based discrimination to include protections on the basis of gender identity and sex stereotypes,” Paschall said. “What this means is that in the context of health care, LGBT people, especially transgender people have now for the first time protections in that setting, which is hugely important.”
Earlier this year, the Department of Health & Human Services issued rules saying that no program activity in an exchange, nor a health plan, can discriminate on the basis of sexual orientation and gender identity. The rule takes effect when exchanges open in 2014.
The administration has taken additional efforts to help the LGBT community when it comes to accessing health care. Same-sex couples can now search for health plans that cover domestic partners through the health care finder tool at healthfinder.gov. HHS has also undertaken data collection efforts to include questions about sexual orientation and gender identity in surveys like the National Health Interview Survey.
Still, advocates are looking for additional efforts from the administration — in addition to the adoption of the Medicaid expansion by the states — to ensure LGBT people are included in health care reform to the greatest extent possible.
Paschall said the Task Force wants to see data collection efforts expanded beyond the federal surveys already designated by the administration.
“Generally speaking, we would like to see sexual orientation and gender identity questions added to all federal surveys where demographic data is collected,” he said. “Our priorities include a number of federal surveys, maybe most notably the American Community Survey, which is an annual survey that collects demographic data and is considered one of the largest annual data sources on the American population.”
For people living with HIV/AIDS, Schmid said he is awaiting from the administration regulatory guidance in the next couple months on essential health benefits to cover people in the Medicaid program and federal exchanges.
“We’ll see if the coverage will be strong enough for medications and for all different other services,” Schmid said.



National
HRC condemns DoE removal of LGBTQ bullying data from federal survey
Organization cites rise in homophobic, transphobic policies, worse mental health outcomes

The Human Rights Campaign is slamming the White House — and the Department of Education — following their removal of some LGBTQ bullying data from federal data collection.
The Civil Rights Data Collection is a mandated survey of all public school districts that collects figures on a wide variety of statistics about students — including demographics that include race, ethnicity, sex, disability status, and English learner status; course-level enrollment data, such as how many students are enrolled in advanced placement or honors classes; and school climate information, such as rates of bullying, harassment, suspensions, and expulsions.
That data collection has been ongoing since 1968 — nearly six decades — but now has a major change in what questions are being asked, or not asked, that advocates are largely attributing to the Trump-Vance administration’s culture war fight on LGBTQ children in the country.
Changes to the 2025-2026 survey questions — approved by the Office of Budget and Management in July — eliminated a space for schools to report how many students identify as nonbinary, how often those students are victims of harassment and bullying, and whether school districts have policies prohibiting gender identity-based incidents.
K-12 Dive, a publication that focuses its reporting on news related to K-12 education, first published a list of these data collection changes from 2024-2025 to 2025-2026.
These questions, as well as others that included LGBTQ student topics on treatment in schools, were added to the CRDC under the Biden-Harris administration. By including these questions, policymakers hoped this would lead to increased investigations into discrimination complaints, initiate compliance reviews, and provide policy guidance to districts, according to Education Department documents.
The CRDC also eliminated the mention of “gender identity” from the definition of rape and sexual assault. The prior collection of data (before the Trump-Vance administration changed it) defined rape as something that could be done to “all students, regardless of sex, or sexual orientation, or gender identity.” Now, the new data collection questions say, “All students, regardless of sex, or sexual orientation can be victims of rape,” removing “gender identity” from the new definition.
By removing and changing definitions, this could have a real-world impact on some of the school’s most vulnerable students. According to CRDC data from 2021-2022, more than 1,800 school districts reported enrolling one or more nonbinary students.
Additional data also shows that the changes to data collection is harming public school students. U.S. Sen. Bernie Sanders (I-Vt.), the ranking member of the Senate Health, Education, Labor, and Pensions Committee released a report in April finding that the Trump-Vance administration’s efforts to all but close the Department of Education Office for Civil Rights has left students facing discrimination and harassment throughout the country without the federal recourse they are entitled to under federal law.
The Williams Institute, a think tank that collects data and conducts research on issues related to sexual orientation and gender identity, has data indicating the true number of nonbinary and transgender children is much higher — they estimate that for children ages 13 to 17, nearly 724,000 identify as nonbinary or trans.
This is in line with a slew of policies pushed by the Trump-Vance administration since their federal takeover. Within his first day in office, President Donald Trump signed Executive Order 14168, titled “Defending Women from Gender Ideology Extremism and Restoring Biological Truth to the Federal Government.” This directive attempts to make the federal definition of gender unchangeable, determined by sex assigned at birth alone.
Within his first month of his second term, Trump issued Executive Order 14187, titled “Protecting Children from Chemical and Surgical Mutilation.” The order directs federal agencies to restrict gender-affirming medical care — including puberty blockers, hormone therapy, and surgeries — for individuals under the age of 19.
He also pushed multiple anti-trans executive orders, including Executive Order 14201, “Keeping Men Out of Women’s Sports,” and Executive Order 14183, “Prioritizing Military Excellence and Readiness,” targeting trans athletes and military members, respectively.
These policies have a real-world impact on trans people.
The Trevor Project, a nonprofit dedicated to crisis and suicide prevention for LGBTQ people under 25, reported that, for the seventh year in a row, LGBTQ youth are at higher risk for suicide as a result of mistreatment and stigmatization.
Trevor Project data showed that nearly 60 percent of LGBTQ young people ages 13-17 said they were bullied in the past year, and that 36 percent of LGBTQ youth seriously considered suicide in the last year. The data shows a bigger discrepancy for trans youth, with that number hovering around 40 percent considering suicide.
HRC President Kelley Robinson issued a statement following the approval of the new data collection questions that leaves LGBTQ students’ bullying statistics under — if not completely unreported.
“If there was even a shadow of a doubt, this latest move by the Trump administration makes it abundantly clear they do not care about the safety of LGBTQ+ students, and trans students in particular,” Robinson said. “These are adults who should be protecting our kids. And instead, they are making sure bullying and harassment are not tracked. If they are not tracked, bullying and harassment cannot be prevented or stopped — which is exactly what the Trump administration wants. Parents deserve to know their kids are safe at school, and every single young person deserves dignity and safety at school. Anything less is plain evil.”
HRC has a “Welcoming Schools” initiative that they say is the “most comprehensive” bias-based bullying prevention program in the nation. The program includes LGBTQ and gender-inclusive resources for schools, help navigating special education and disability resources for LGBTQ-identifying students, and other tools to help schools become more inclusive.
This program has been in effect for nearly two decades and, according to HRC, reaches nearly 750,000 students.
The Washington Blade reached out to both the Department of Education and Office of Management and Budget for comment but did not receive a response by publication time.
Michigan
Progressives score victory as El-Sayed wins Mich. Senate primary
Democratic newcomer will face Rogers in November

Michigan held its primary on Tuesday, allowing the two major political parties to select their nominees to go head-to-head for the state’s U.S. Senate seat.
NBC News called the Democratic race early, giving the victory to physician Abdul El-Sayed over incumbent U.S. Rep. Haley Stevens (D-Mich.) in an extremely close primary. El-Sayed won 48.5 percent of the primary vote, with Stevens trailing by just one percentage point at 47.5 percent.
Both candidates have campagined on supporting the LGBTQ community through different avenues— for El-Sayed he focused on his past promoting HIV and PrEP funding and research. Stevens focused on her legislative history working to support transgender rights in the state.
This is a major win for progressive Democrats, who have been bearing the brunt of political attacks from President Donald Trump, the Republican Party, and centrist Democrats.
El-Sayed, a former health director in Detroit, ran his campaign largely on making life in the Great Lakes State more affordable amid rising costs. His policies include promoting “Medicare for All,” pushing health policy that targets the regressive efforts of the Trump-Vance administration that rolls back funding for both Women and LGBTQ people, minimizing the growing amount of money in politics, and he was very vocal in his criticism of Stevens for supporting aid to Israel. He was endorsed by two major progressives — U.S. Sen. Bernie Sanders (I-Vt.) and U.S. Rep. Alexandria Ocasio Cortez (D-N.Y.).
Stevens, the four-term congresswoman, is much closer to establishment Democrats on policy than El-Sayed.
During her time in the federal government, she has consistently supported the Equality Act, which would add sexual orientation and gender identity as protected classes under the Civil Rights Act of 1964. She has also emphasized supporting local manufacturing and lowering housing costs in the state.
She was named to Advocates for Trans Equality’s 118th Congressional Champions list for her pro-trans policies and was endorsed by establishment heavy hitters Michigan Gov. Gretchen Whitmer and Senate Minority Leader Chuck Schumer (D-N.Y.).
The contentious race boiled down not only to Michigan affairs but also extended to international conflicts — namely Palestine. (South Africa has filed a case in the International Court of Justice in The Hague that accuses Israel of committing genocide in the Gaza Strip after Oct. 7.) This primary also acted as one of the first major races that pushed back against AIPAC, a lobbying group that works to promote pro-Israel candidates in U.S. elections. The group has been involved in domestic politics since 1954.
AIPAC devoted a massive amount of money to this race.
The Associated Press reported that the pro-Israel lobbying group spent more than $30 million on ads against El-Sayed because of his vocal denunciation of Israel and his continued criticism of its policies towards Palestine.
Michigan has a large Muslim and Arab American population, which could, in part, explain how El-Sayed was able to win.
The Republican side was far less competitive. Former U.S. Rep. Mike Rogers (R-Mich.) ran unopposed and clinched the GOP nomination. He has consistently held anti-LGBTQ positions, going as far as voting multiple times for a federal constitutional amendment to ban same-sex marriage, voting against repealing the military’s “Don’t Ask, Don’t Tell” policy, and supporting efforts to directly target the attempted expansion of Title IX protections to include trans people.
El-Sayed will face off against Rogers in November for Michigan’s Senate seat — one that could have lasting impacts not only on the state’s politics but also on the Republicans’ narrow Senate majority and Trump’s political agenda.
National
White House orders warning signs at Smithsonian over gender identity exhibits
Administration criticizes National Museum of American History

The Trump administration will install temporary warning signs outside the Smithsonian’s National Museum of American History after releasing a report accusing the museum of promoting what it calls “radical” gender ideology and other politically biased content.
According to the Executive Order, “For purposes of policy formulation under EO 14253, this review of the National Museum of American History concludes that NMAH, by the intention and at the direction of current Museum and Smithsonian leadership, has become subject to institutional capture by a radical, activist ideology that is fundamentally opposed to telling the noble, honest story of the great country we know and love.”
Executive Order 14253 refers to what the White House has deemed the “Restoring Truth and Sanity to American History” order. Therefore, the Trump administration has said it will take all available steps to ensure that the issues in the report are addressed and rectified.
Without specifying, the White House has stated that warnings will be posted along NMAH to alert visitors to sections of the museum it has deemed are in violation according to the report.
“The Secretary of the Interior, acting through the Director of the National Park Service (NPS) and in coordination with the Assistant to the President for Domestic Policy, shall install temporary signage along the NPS-maintained sidewalks and walkways used by the public to access the Museum, informing visitors of the findings of the Report and of the policy set forth in section 1 of this order,” the Executive Order states.
The warnings were raised in a 162-page report issued by the Domestic Policy Council. The report detailed ways in which the National Museum of American History (NMAH) has “poorly” portrayed American history and insufficiently highlighted the founding story during America 250th celebrations.
The report outlined key findings of the NMAH. One of these findings was the Center for Restorative History within the museum, which has stated its purpose is to “encourage systemic change” by highlighting diverse groups. However, the report states that it highlights every group of Americans except for straight and white Americans.
The Domestic Policy Council accused the museum of engaging in “transgender activism.” According to the report, examples include referring to “biological men” as women or girls, displaying what it describes as sexually suggestive content, and incorporating discussions of gender fluidity, gender identity, and gender nonconformity into the museum’s educational curriculum, “Becoming US.”
The report also criticizes the curriculum for using the term “transgender” when discussing gender-nonconforming people and encouraging individuals to ask a person’s pronouns when meeting them. It further objects to exhibits stating that “transgender, nonbinary, and cisgender female athletes” continue to struggle for and demand equality.
It also condemns what it refers to as explicit content in an exhibition, “Girlhood (It’s Complicated)”, such as chest binders, questioning gender testing in women’s sports, and referring to biological females as “people inhabiting female bodies.”
Additionally, the report accuses the museum of no longer participating in flag-celebrating ceremonies because it was “too busy” preparing for June Pride and WorldPride events. It states, “As Director Hartig explained in a June 2024 presentation, all her attention was focused on flying the Smithsonian Pride Alliance’s ‘intersexual pride flag during June’ in 2023 and 2024.”
On July 9, the American Historical Association issued a statement rejecting the report’s findings.
In regard to the report, it states, “Its anonymous authors overlook a central lesson of the nation’s founding: the United States was forged by finding common purpose amid intense divisions, conflicts, and disagreements.” They argue that only “honest history” can tell the true history of the nation.
House Republicans led a subcommittee hearing that questioned Smithsonian Director Hartig extensively. A main focus of the questions was on the exhibits related to gender identity and whether they were appropriate. In the hearing, Rep. Nancy Mace asked: “When was your gender revealed to you, Dr. Hartig?”
In response to questioning, Hartig stated that the institution is nonpartisan and does not push a specific agenda.
Hartig published a two-page statement ahead of her hearing outlining her thoughts on the situation. In the report, she states that the institution is always open to criticism and will continue to look for ways to improve, but she sees the report as misleading.
“I can attest that the report does not fairly characterize the full body of work at this museum. I am familiar with the depth and breadth of our collections, exhibits, and programming. And while I recognize there is always room for improvement, I also know the beauty, inspiration, and expertise that exists in our museum,” Hartig wrote.
Democrats created their own 16-page report as a rebuttal to the Domestic Policy Council’s report. It argued that the attacks by the current Trump administration are another example of its attempt to rewrite history. Additionally, the report states that no policy changes were included in the Executive Order, as that is beyond the President’s role. “The Report recommends nothing. That is no accident. To recommend an action, the Report would need to identify who is legally empowered to take it, and its own opening chapter concedes the President’s only power is to ‘urge’,” House Democrats wrote.
It is still unclear when the temporary warnings will be installed or what form they will take beyond the requirements outlined in the executive order.
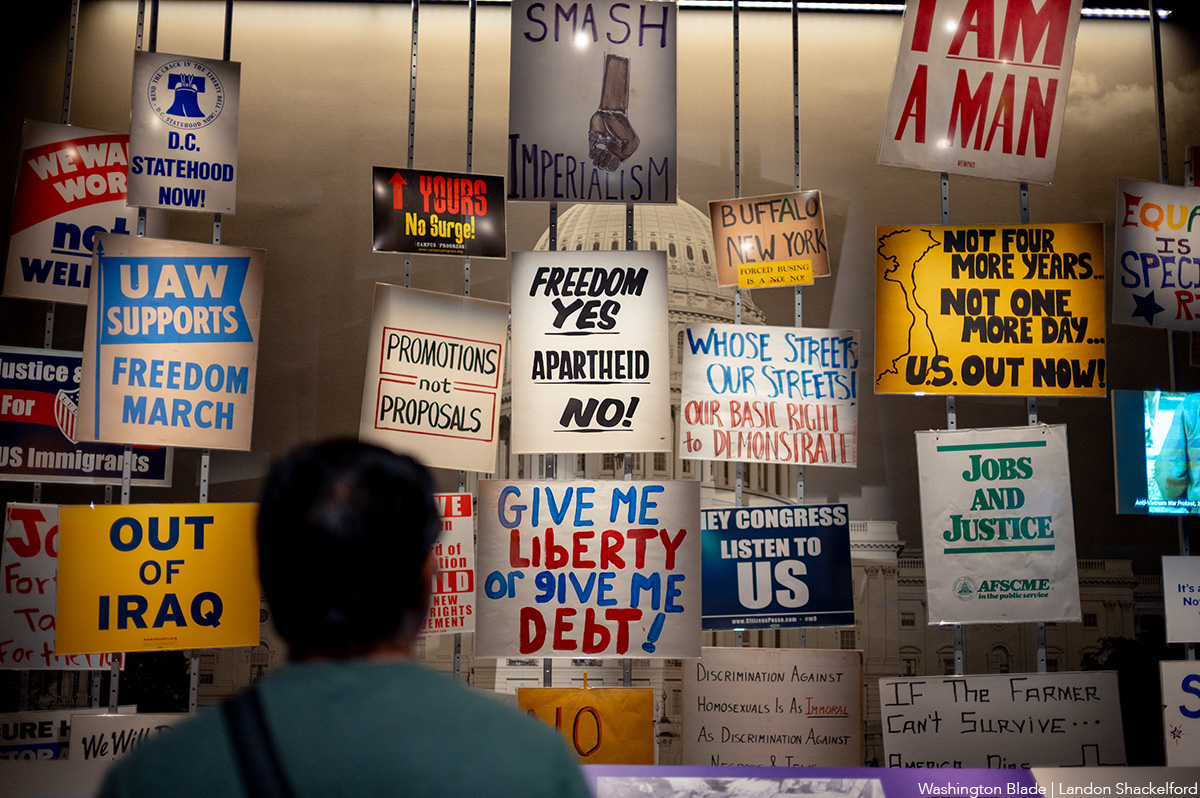
An exhibit at the Smithsonian. (Washington Blade photo by Landon Shackelford)

PHOTOS: World Pride March

Tens of thousands take part in World Pride March

PHOTOS: Daddy Issues at Kiki

Something’s off about Dad. When is it time to step in?

New book chronicles gay man’s life in hippie commune

Progressives score victory as El-Sayed wins Mich. Senate primary

Doug Ollivant to face Eugene Vindman in Va. 7th Congressional District

LGBTQ advocates optimistic about D.C.’s expected new mayor

Continue to engage in community after Pride month

D.C.’s Mary’s House For Older Adults names new executive director
-

 Michigan5 days ago
Michigan5 days agoProgressives score victory as El-Sayed wins Mich. Senate primary
-
Virginia5 days ago
Doug Ollivant to face Eugene Vindman in Va. 7th Congressional District
-
District of Columbia5 days ago
LGBTQ advocates optimistic about D.C.’s expected new mayor
-
Opinions4 days ago
Continue to engage in community after Pride month


