National
Meet the new faces of LGBT juvenile corrections
DOJ, municipalities and former inmates are working to save gay youth


Lorie Brisbin, a program specialist with the Department of Justice, said many LGBT juveniles in custody are there for survival crimes. (Photo courtesy of DOJ)
By THOM SENZEE
LGBT youth have enough trouble adjusting to life in what is still, for lack of a better term, “a straight man’s world.” But for LGBT youth in custody, the world is often a supremely frightening place.
“There is a significant portion of LGBTI juveniles in custody who are there for what we can call survival crimes,” explains Lorie Brisbin, a program specialist with the Department of Justice’s Office of Juvenile Justice and Delinquency Prevention (OJJDP).
“In many cases, these are kids who have been kicked out of their homes by their families simply because of their particular orientation, be that lesbian, gay or what have you.”
Made homeless by their parents as adolescents or as teenagers, and forced to face a tough world on their own with no basic tools for living—such as work experience or identification cards—some LGBT youth turn to petty crimes in order to survive. Survival crimes range from stealing food from grocery stores to prostitution and burglary.
In fact, merely being a homeless minor after 10 p.m. amounts to a violation of curfew laws, not to mention truancy if they cannot stay in school after becoming homeless.
Of course, some homeless youth turn to more serious crimes. Regardless of how they end up in custody, LGBT juveniles find themselves in a system that is only now beginning to recognize that there is a difference in needs compared to their heterosexual counterparts that corrections officials must know in order to keep them safe and well.
“Corrections is a very closed system,” Brisbin said. “There is a lot of education that needs to go on in helping staff feel comfortable with certain issues.”
Two specific issues that could be considered the meat and potatoes of the over-arching problem of how to safely and healthfully manage LGBT juvenile inmates are isolation and gender-appropriate placement.
Getting those two issues right, according to experts, builds a foundation where both juveniles in custody and corrections staff are safer than they would be otherwise.
“For instance, if you have a gay male who is not willing to hide who he is—and most are more than willing to hide—the way it used to work, staff were traditionally going to isolate you for your own protection,” explained Laura Garnette, deputy chief probation officer at Santa Clara County, Calif. Juvenile Detention Division.
“But the courts have said that’s unconstitutional. And actually I say to them, corrections staff, that’s your job. It’s not the juvenile’s job to keep himself safe; that’s what you’re getting paid to do. You’re making them do your job by putting them in isolation.”
According to OJJDP’s Brisbin, Garnette’s employer is a model of safety, efficacy and ethical management of LGBT and intersex juveniles in custody.
“Santa Clara County is phenomenal,” Brisbin told the Washington Blade. “It starts with their perspective, looking at their policies and making their environment safer and more welcoming.”
“More welcoming” might sound like an odd phrase to use when talking about incarceration. But it is important to remember, according to Brisbin, as well as Deputy Chief Probation Officer Garnette and other corrections professionals the Blade spoke to in researching this story; juvenile detention is mandated to rehabilitate rather than simply punish, as is often the case in adult corrections systems.
“Santa Clara probation has worked hard to redefine juvenile corrections,” said Brisbin, speaking by phone from her office at the Department of Justice in Washington, D.C. “Now, when a youthful offender who is lesbian, gay, bisexual, transgender or intersex comes in, they are processed much differently, providing the best possible outcome for the general population and the staff.”
But it is not necessarily easy to bring change to the corrections establishment.
“You want to watch something entertaining, just tell a group of unenlightened corrections workers that they need to put a male-to-female transgender offender into housing with girls,” Santa Clara County’s Garnette said. “You’d think you had just told them the most hilarious or outlandish thing anyone ever said.”
Nowadays all youthful offenders in Santa Clara County are processed into and counseled within custody in a manner that is both neutral in terms of sexual orientation and gender identity.
“For instance, I might ask a male inmate if he has a girlfriend or if he has a boyfriend,” explains Garnette. “He might respond, ‘why would you ask me if I have a boyfriend; what do you think I am a fucking faggot?’”
“And then, of course, I respond, ‘well, why wouldn’t I ask? You could have either. How would I know which? There are plenty of gay young men who don’t fit stereotypes.’”
According to Garnette, that response safely opens the door for an honest answer if the youth is gay, while also planting a seed of tolerance if he is straight.
Santa Clara County neither isolates LGBT juvenile inmates individually, nor places them together in separate groups. Instead, officials and detention staff work with vigilance by observing and counseling all inmates to prevent physical altercations and eliminate bullying in real time—on the floors of housing units in its detention centers, 24/7.
“Isolation is not the solution,” Garnette said. “It’s our job to keep these kids safe by using our words, our eyes and our ears. Yes, it’s hard work, but simply isolating them is lazy and injurious. If you can’t do the job of keeping gay kids safe in the general population, then I’m sorry; get a different job.”
According to OJJDP’s Brisbin, a new vigor arrived in the juvenile corrections profession when, in 2012, the Justice Department issued national standards for ensuring that detention facilities conform to the 2003, “Prison Rape Elimination Act” (PREA) for the first time.
Among a litany of guidelines announced by Attorney General Eric Holder was a mandate to “incorporate unique vulnerabilities of lesbian, gay, bisexual, transgender, intersex and gender nonconforming inmates into training and screening protocols.”
Brisbin organizes workshops for corrections officials and juvenile detention facilities workers around the nation. Her training sessions are designed to introduce technical tools to help realize the promise of PREA, which is an end to rape and sexual abuse behind bars.
“For example PREA calls for changes in language that has been used in facilities in the past,” Brisbin said. “We talk about respectful communications—how do you do it and still get the kind of behavior you need for conformity in a locked-down situation.”
According to her, the words once used recklessly by officials at juvenile lockdowns can actually incite abuse.
“But words can also help prevent violence,” she said. “If you have a verbally disrespectful environment, that can be very, very unsafe. Don’t use terms that are inherently offensive. For instance, it used to be respectful to use the term hermaphrodite; that’s no longer seen as acceptable to use.”
Transgender and intersex youth in custody face particularly tough circumstances finding their places in detention settings. However well intentioned, detention-facility staff with varying levels of education can find the task of helping transgender, questioning and intersex youth safely fit in at “juvie” quite daunting.
Consider the latter of those three categories of youth: The Intersex Society of North America says the complexity of intersexuality makes it a subjective issue—albeit with real biological (i.e., chromosomal and genitalia-related) aspects.
“[Intersexuality] is a socially constructed category that reflects real biological variation,” reads the introductory statement on the group’s homepage. “To better explain this, we can liken the sex spectrum to the color spectrum. There’s no question that in nature there are different wavelengths that translate into colors most of us see as red, blue, orange, yellow. But the decision to distinguish, say, between orange and red-orange is made only when we need it—like when we’re asking for a particular paint color…”
When even experts and advocates admit that making gender distinctions among intersex persons can be similar to knowing the difference between burnt-orange and maroon-rust, how is a juvenile hall counselor working the graveyard shift in a Midwest suburb supposed to know how to refer to an intersex juvenile inmate?
The answer, according both Brisbin and Garnette, is surprisingly simple—let the individual inmate decide. They say the same rule applies to transgender youth in custody.
“The very worst thing you can do is call a transgender girl ‘he’ or ‘him,’” she said. “Not only can that lead to violence from other inmates, which puts the staff in danger as well as the kids in the facility, but it’s emotionally violent. It does real harm.”
Garnette, who is a lesbian, entered the corrections field at the end of the 1980s.
“It was about as different then compared to today as you can imagine,” she said. “This is an exciting time to be working in this field. In the past 10 years we have seen a change to evidence-based policies and procedures that wasn’t there before.”
According to Garnette, there was a time in her early career when she had bosses whose approaches to juvenile corrections were strictly tough for sake of toughness, or more permissive simply for the sake of permissiveness.
“Either way, it wasn’t about using research for evidence-based outcomes,” she said. “Now it’s exactly the opposite; that’s just what we do.”
Ten years ago it might have been impossible for Mark Seymour, a former inmate who served time in prison for a drug offense, to work with leading practitioners and researchers in the juvenile corrections field.
“When I got out of prison in 2010, I knew I wanted to do something to make it better for LGBT youth in custody because I know first-hand how bad things like being put in isolation—just because you happen to be gay—can be,” Seymour told the Blade. “It took everything I had within me to not lose my mind in isolation.”
Seymour is the first fellow at the National Center for Youth in Custody. He is currently helping implement a pilot program to disseminate the fast-growing body of evidence-based knowledge about how to better meet the stated missions of juvenile corrections facilities: rehabilitating youthful offenders.
“The exciting thing is that a big part of this new push to bring scholarship, research and practical knowledge about what works is a focus on LGBTI kids,” explains Seymour. “The youth of our community, for the first time, are part of the conversation.”






National
White House orders warning signs at Smithsonian over gender identity exhibits
Administration criticizes National Museum of American History

The Trump administration will install temporary warning signs outside the Smithsonian’s National Museum of American History after releasing a report accusing the museum of promoting what it calls “radical” gender ideology and other politically biased content.
According to the Executive Order, “For purposes of policy formulation under EO 14253, this review of the National Museum of American History concludes that NMAH, by the intention and at the direction of current Museum and Smithsonian leadership, has become subject to institutional capture by a radical, activist ideology that is fundamentally opposed to telling the noble, honest story of the great country we know and love.”
Executive Order 14253 refers to what the White House has deemed the “Restoring Truth and Sanity to American History” order. Therefore, the Trump administration has said it will take all available steps to ensure that the issues in the report are addressed and rectified.
Without specifying, the White House has stated that warnings will be posted along NMAH to alert visitors to sections of the museum it has deemed are in violation according to the report.
“The Secretary of the Interior, acting through the Director of the National Park Service (NPS) and in coordination with the Assistant to the President for Domestic Policy, shall install temporary signage along the NPS-maintained sidewalks and walkways used by the public to access the Museum, informing visitors of the findings of the Report and of the policy set forth in section 1 of this order,” the Executive Order states.
The warnings were raised in a 162-page report issued by the Domestic Policy Council. The report detailed ways in which the National Museum of American History (NMAH) has “poorly” portrayed American history and insufficiently highlighted the founding story during America 250th celebrations.
The report outlined key findings of the NMAH. One of these findings was the Center for Restorative History within the museum, which has stated its purpose is to “encourage systemic change” by highlighting diverse groups. However, the report states that it highlights every group of Americans except for straight and white Americans.
The Domestic Policy Council accused the museum of engaging in “transgender activism.” According to the report, examples include referring to “biological men” as women or girls, displaying what it describes as sexually suggestive content, and incorporating discussions of gender fluidity, gender identity, and gender nonconformity into the museum’s educational curriculum, “Becoming US.”
The report also criticizes the curriculum for using the term “transgender” when discussing gender-nonconforming people and encouraging individuals to ask a person’s pronouns when meeting them. It further objects to exhibits stating that “transgender, nonbinary, and cisgender female athletes” continue to struggle for and demand equality.
It also condemns what it refers to as explicit content in an exhibition, “Girlhood (It’s Complicated)”, such as chest binders, questioning gender testing in women’s sports, and referring to biological females as “people inhabiting female bodies.”
Additionally, the report accuses the museum of no longer participating in flag-celebrating ceremonies because it was “too busy” preparing for June Pride and WorldPride events. It states, “As Director Hartig explained in a June 2024 presentation, all her attention was focused on flying the Smithsonian Pride Alliance’s ‘intersexual pride flag during June’ in 2023 and 2024.”
On July 9, the American Historical Association issued a statement rejecting the report’s findings.
In regard to the report, it states, “Its anonymous authors overlook a central lesson of the nation’s founding: the United States was forged by finding common purpose amid intense divisions, conflicts, and disagreements.” They argue that only “honest history” can tell the true history of the nation.
House Republicans led a subcommittee hearing that questioned Smithsonian Director Hartig extensively. A main focus of the questions was on the exhibits related to gender identity and whether they were appropriate. In the hearing, Rep. Nancy Mace asked: “When was your gender revealed to you, Dr. Hartig?”
In response to questioning, Hartig stated that the institution is nonpartisan and does not push a specific agenda.
Hartig published a two-page statement ahead of her hearing outlining her thoughts on the situation. In the report, she states that the institution is always open to criticism and will continue to look for ways to improve, but she sees the report as misleading.
“I can attest that the report does not fairly characterize the full body of work at this museum. I am familiar with the depth and breadth of our collections, exhibits, and programming. And while I recognize there is always room for improvement, I also know the beauty, inspiration, and expertise that exists in our museum,” Hartig wrote.
Democrats created their own 16-page report as a rebuttal to the Domestic Policy Council’s report. It argued that the attacks by the current Trump administration are another example of its attempt to rewrite history. Additionally, the report states that no policy changes were included in the Executive Order, as that is beyond the President’s role. “The Report recommends nothing. That is no accident. To recommend an action, the Report would need to identify who is legally empowered to take it, and its own opening chapter concedes the President’s only power is to ‘urge’,” House Democrats wrote.
It is still unclear when the temporary warnings will be installed or what form they will take beyond the requirements outlined in the executive order.
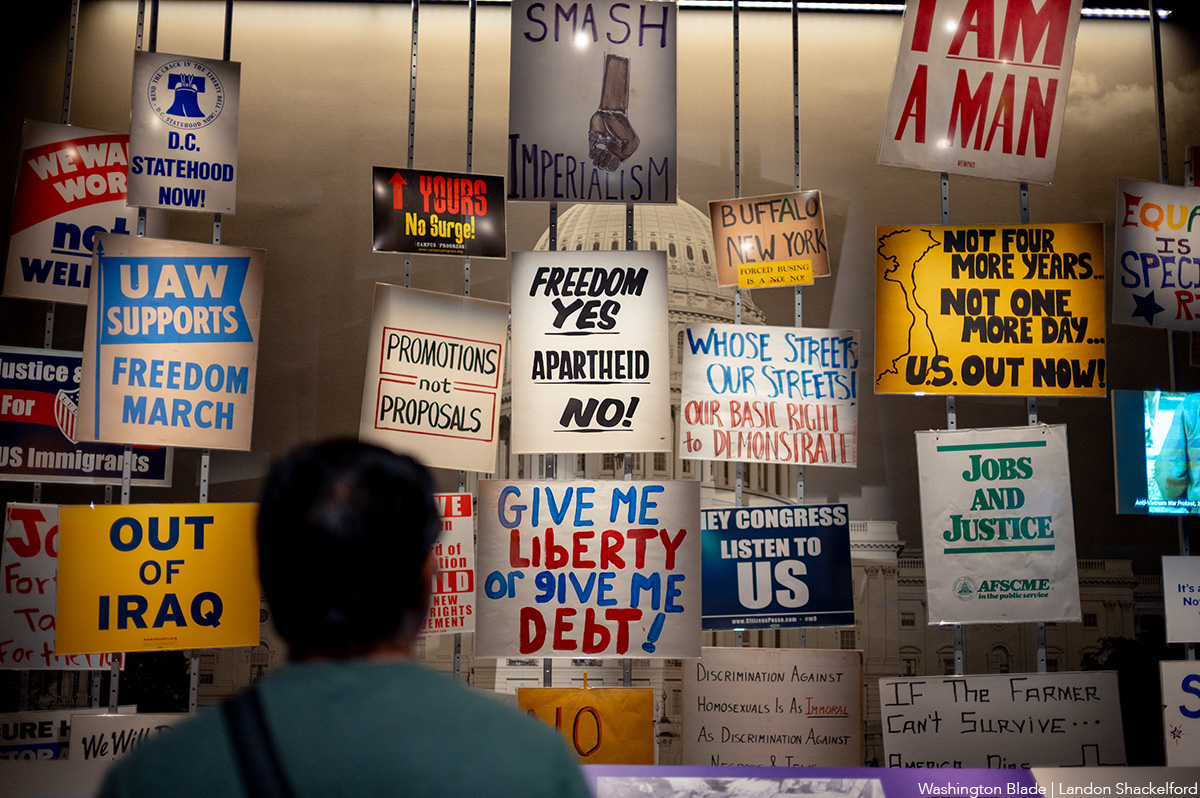
An exhibit at the Smithsonian. (Washington Blade photo by Landon Shackelford)
National
Trump ends direct HIV prevention funding to community groups
Advocates say transfer of funds to states may disrupt local programs

A decision by the U.S. Office of Management and Budget (OMB) at the request of the Trump administration to discontinue direct federal funding of community-based organizations and clinics that provide HIV prevention services has raised concern among community health advocates, including LGBTQ advocates.
News surfaced earlier this month that the OMB informed the U.S. Centers for Disease Control and Prevention that it would not renew $46 million in funding for 96 community-based organizations that provide HIV testing, referrals to medical care, and arrangements for obtaining pre-exposure HIV prevention medication known as PrEP that has been shown to be 99 percent effective in preventing HIV infection.
Under the new policy arranged by OMB, the funds will be redirected to the states to be allocated to state and local health departments. The policy calls for states to encourage but not require their respective state and local health departments to allocate some of those funds for community-based organizations. Under the new policy, the funding is scheduled to last until May of 2027, before a renewal decision is made.
Some political observers have speculated that the decision to end direct federal funding to community-based organizations could be motivated by the Trump administration’s hostility to diversity, equity, and inclusion or DEI programs and organizations that promote those programs, with the belief that some of the groups receiving the federal HIV prevention funds are promoting DEI.
Carl Schmid, executive director of the D.C.-based HIV+ Hepatitis Policy Institute, is among the leaders of many AIDS advocacy organizations expressing strong opposition to the OMB action. Schmid said that in places like D.C. and some states, local officials will be willing to redirect the federal funds to local community-based organizations.
A list of the 96 community-based organizations across the country that are currently receiving the federal AIDS funds includes the D.C.-based Whitman-Walker Health, which has a long history of healthcare support for the LGBTQ community, and La Clinica del Pueblo, which reaches out to the Latino community.
Schmid said Whitman-Walker and La Clinica del Pueblo have longstanding good relationships with the local D.C. government.
“But other states and jurisdictions don’t have that relationship with the community-based organizations,” Schmid said. “It depends on the state,” he said, adding, “Not all states send their money to the communities that really need it most. And not all states are fast in getting money to the community-based organizations.”
Spokespersons for Whitman-Walker and La Clinica del Pueblo couldn’t immediately be reached for comment on whether they think the Trump administration’s latest action related to funding will adversely impact their respective organizations.
Schmid said under the current federal grant program slated to be discontinued, which has been in effect for at least five years, HIV-related health organizations receiving the federal grant funds were eligible for an existing federal policy enabling them to purchase HIV-related medication, including the PrEP prevention medication, at a significant discount from pharmaceutical companies. With the ending of the direct federal HIV funds to community-based organizations, Schmid said it was unclear whether problems may surface in obtaining drug discounts.
“They could still qualify as a sub-grantee from a state,” Schmid said. “But what if they don’t get that grant again? They would not be able to qualify to obtain the drugs” at the discounted price, he said.
Among the organizations expressing strong concern over the decision to discontinue the direct HIV prevention funding to community-based organizations has been the Federal AIDS Policy Institute and its subgroup called the HIV Prevention Action Coalition.
In a July 22 letter bearing the names of 71 community-based organizations from throughout the country sent to U.S. Department of Health and Human Services Secretary Robert F. Kennedy Jr. and Centers for Disease Control and Prevention Acting Director Jay Bhattacharya, the group called for the Trump administration to “reconsider” ending the current funding policy.
“Ending this program without a clear plan for what comes next would dismantle prevention infrastructure that has taken more than three decades of federal investment to build and do so just as that long record of measurable returns is accelerating,” the letter states.
It says the initiative by President Trump in his first term as president to end the HIV epidemic and reduce new HIV infections by 90 percent by 2030 was moving ahead by the funding program for community-based organizations that the administration now wants to end.
“Discontinuing this program would also cost far more than it saves,” the letter says. “Every HIV transmission prevented avoids an estimated lifetime treatment cost of roughly half a million dollars per person to the healthcare system – costs that fall heavily on taxpayer-funded programs, including Medicaid, Medicare, and the Ryan White HIV/AIDS program,” the letter continues.
“The choice before the administration is straightforward: a modest, targeted investment in prevention now, or far greater public expense for treatment later,” the letter concludes.
Spokespersons for the OMB and the Department of Health and Human Services, which oversees the CDC, have not immediately responded to news media requests for comment on the opposition to the funding change policy.
National
At Alliance Defending Freedom’s summit, church and state are one
House Speaker Mike Johnson (R-La.) among speakers

Uncloseted Media published this article on July 23.
By SPENCER MACNAUGHTON | Earlier this month, hundreds of people filled a conference room in San Diego. These included Speaker of the House Mike Johnson, Assistant Secretary of Health Admiral Brian Christine, OpenAI executive Dean Ball, and the attorneys general of West Virginia and Idaho.
They all came together for Alliance Defending Freedom’s 2026 Summit. The Christian legal group, also a Southern Poverty Law Center-designated anti-LGBTQ hate group, described the event as a “gathering of leaders from many different spheres, including law, public policy, media, business, education, and Christian leadership.”
Johnson — who has said that “homosexual relationships are inherently unnatural and … society cannot give its stamp of approval to such a dangerous lifestyle” — was a featured speaker.
In his speech, he seemed unconcerned with the separation of church and state: “It is so encouraging to Kelly and I to be among friends and fellow warriors for this cause and people who understand that God is not done with America yet. … ADF’s on the very tip of the spear, front line, defending those very truths and keeping the door open for the spread of the Gospel. This is our moment. I’m telling you, I believe the next season … is going to be the greatest season of this ministry since its inception.”
That ministry is one that has espoused aggressively anti-LGBTQ views since its inception in the early 1990s. It was co-founded by a group of evangelical men, including Alan Sears, who co-authored a book called “The Homosexual Agenda: Exposing the Principal Threat to Religious Freedom Today.” Since then, ADF has opposed gay marriage and supported bans on gay sex and on gender-affirming care for minors.
After helping overturn Roe v. Wade, ADF lawyers have led key victories at the Supreme Court. In 303 Creative v. Elenis, SCOTUS ruled that a website designer could refuse service to gay weddings. And this year they convinced the Court to overturn Colorado’s ban on conversion therapy and to uphold state laws in West Virginia and Idaho that ban trans girls from playing on girls’ sports teams.
At the summit, ADF President Kristen Waggoner, who has promoted conversion therapists and consistently misgenders trans people, interviewed these states’ attorneys general.
“The lawyers who were defending women’s sports were among the best I’ve ever seen in my entire life,” West Virginia Attorney General JB McCuskey told Waggoner.
Similar to Johnson, Trump’s Assistant Secretary of Health Christine showed his commitment to governing based on conservative Christianity. He gave a Bible-thumping speech against gender transition and trans healthcare, saying that it “contradicts … the deeper moral order that is woven into creation itself. For Genesis 1:27 informs us that God created man in his own image. … Male and female” He also said the “complementary relationship between man and woman is divine” and advocated for youth with gender dysphoria to receive care from a pastor.
All of these remarks from politicians made me think of the interview I published earlier this week with Pete Hegseth’s pastor, Doug Wilson. He wants a Christian theocracy in America and told me that: both the perpetrator and the victim should be disciplined in some cases of marital rape; that transgender people are “sad;” that execution is justifiable for certain homosexual acts; and that gay sex should be illegal.
The ADF Summit is glossy and polished. And while its messaging may be less explicit than Pastor Wilson’s, the track record of the organizations shows they have the exact same desires. They’re just deeply strategic in what they say and when and how they say it.
I believe the political power players who attended this year’s summit know this. They know they are endorsing an organization whose members have essentially called for the illegalization of most — if not all ‚ forms of queer behavior and presentation.
In the last few years, these perspectives have become increasingly embedded in the highest rooms of the federal government and they have been effective in stripping away LGBTQ rights. Wilson, who just installed a full-time pastor in Washington to lead services, says there are 10 to 20 government officials who align with his church’s ideology.
It is vital for Americans to keep their eyes wide open to the ultimate goal of groups like ADF: to create a United States that leaves LGBTQ people without rights and that pushes us back in the closet.

PHOTOS: Petal Release Party

Madonna headlines World Pride Music Festival in Amsterdam

Reggie White relishing first season as artistic director of Woolly Mammoth

PHOTOS: Amsterdam Pride Canal Parade

Amsterdam Pride Canal Parade draws hundreds of thousands

‘Heartstopper Forever’ delivers satisfying conclusion

Madonna to perform at World Pride in Amsterdam

BLADE ENDORSEMENT: Susan Stewart for mayor of Rehoboth Beach

PHOTOS: Lambda Legal in the Pines