Opinions
Medicaid cuts will lead to an uptick in STIs
Move threatens progress to end HIV epidemic
We have come a long way from the days when HIV was an almost certain death sentence. But our work is far from over. The COVID-19 pandemic led to an uptick in rates of sexually transmitted infections (STIs), including HIV, and low-income communities, LGBTQ+ communities, and communities of color continue to be impacted at alarming and disproportionately high rates.
These communities are also more likely to be served by Medicaid. Medicaid is the largest source of insurance coverage for people living with HIV in the United States, covering an estimated 40 percent of nonelderly adults with HIV, and Medicaid accounted for 45 percent of all federal HIV spending in 2022. During September, Sexual Health Awareness Month, it is worth examining the crucial ways Medicaid works to keep people healthy — and what threatens our progress today.
In recent weeks, we have seen a troubling trend develop. Five million Americans have been removed from Medicaid rolls, and many millions more are on the verge of losing coverage as a result of the Medicaid enrollment cuts. This represents the single greatest threat to our progress toward ending the HIV epidemic in years.
During the pandemic, Medicaid enrollment grew by an estimated 20 million people, contributing to the uninsured rate dropping to the lowest level on record in early 2022. But, after a three-year period during which states provided continuous enrollment in exchange for enhanced federal funding, some states resumed dis-enrolling people from Medicaid on April 1. A recent KFF survey found that 17 million people could lose Medicaid coverage as a result of this process, referred to as the Medicaid “unwinding.”
Many states are not doing enough to ensure that Medicaid-eligible residents don’t lose their coverage. While some have been removed from the rolls because they are newly ineligible, procedural issues account for 74 percent of people losing coverage. An unacceptably high number of Florida, Texas, and Virginia residents who are still eligible for Medicaid are losing coverage because of procedural reasons, such as failing to confirm proof of income or household size.
Our goal should be to ensure that no one who qualifies for Medicaid loses their coverage. The U.S. Centers for Medicare and Medicaid Services (CMS) gave states the option to use a 12-month grace period, along with other flexibilities, to prepare for the unwinding and make sure residents had what they needed to recertify. So why are some states so eager to remove their residents from Medicaid rolls?
New York, on the other hand, has made equity a cornerstone of recertification work and provides a template for what states can do to help their residents remain covered. The state maximizes the flexibilities offered by CMS and works directly with providers, health plans, and recipients to minimize procedural disenrollments and ensure that people retain health care coverage, either through Medicaid, the state’s health exchange, or private insurance. New York is among the nation’s top-performing states in terms of call center wait times, call drop rates, and average time it takes to make an eligibility determination, according to the Center on Budget and Policy Priorities. New York’s call center is also able to produce materials in 26 languages. In June 2023 alone, New York State certified renewals for more than 400,000 residents.
At Amida Care in New York, we know firsthand that gaps in care for people living with or placed at elevated risk of contracting HIV can be especially devastating. When people lose access to PrEP medication to prevent HIV, they are left vulnerable to contracting HIV, and when people living with HIV lose access to antiretroviral therapy, they risk becoming seriously ill and transmitting HIV to others. We support and guide our members through the recertification process with dedicated outreach efforts that include phone calls, mailings, text messages, and home visits to limit loss of coverage and interruptions in life-saving treatments.
We cannot begin to address health inequity or end the HIV epidemic without strengthening Medicaid. The recent moves by some states to strip their residents of Medicaid coverage will undermine the progress we’ve made.
Doug Wirth is president and CEO of Amida Care, a Medicaid Special Needs Health Plan for people affected by HIV.






Opinions
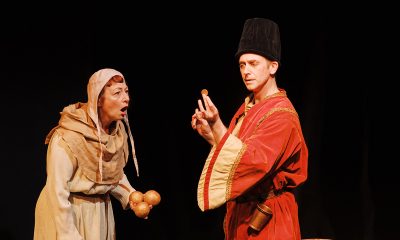
Matthew Rosenstein in ‘Make Me French’ a hit at Clear Space Theatre
‘A bagel who dreamed of being a croissant’

Clear Space Theatre Company was founded in 2004 and has become a huge success in Rehoboth Beach, Del. They present performances all year long, and always have a great summer season when the town grows by the thousands. Not only do they have some great main productions this year, “The Cher Show,” “Pretty Woman,” and “Mean Girls,” but they also have a strong series of cabaret performances.
Matthew Rosenstein’s show, “Make Me French!” was part of that series. While I haven’t seen them all, it will be hard to beat his show. He is a superb storyteller and singer. He blends his real-life experiences, with music from different genres, including showtunes and French disco. Some of the songs he uses to tell his story include: “Belle / Go the Distance” (Menken/Ashman; Menken/Zippel), “Ahh, Paree/Les prénoms de Paris” (Sondheim; Brel); and “Hymne à L’Amour” (Marguerite Monnot/Edith Piaf/Hiroyuki Takei/Fumiaki Uemura).
He has a way of making you feel part of his life story. The show is directed and co-authored by cabaret icon Robbie Rozelle, and it features music direction and arrangements by the incredibly talented Michael Cuschieri, who also plays the piano. The backup band included, Jim McGiffin on bass; Joshua Getka on drums; and Jessica Brams-Miller who sings backup and banters with Matthew, in a wonderful French accent. They are all immensely talented.
The blurb I received from Clear Space said about the show: “A bagel who dreamed of being a croissant, young Matt Rosenstein longed for a life that was far more sophisticated, and interesting, than his own as a suburban New Jersey teenager in the 1990s. His one prayer? “Make Me French!” Matt was determined to not just learn French but to be as French as possible.” Matt went so far as to call Air France from pay phones as a youngster, just to practice speaking with a real French person.
He eventually got the chance to move to Paris to fulfill his dream, and learned some hilarious lessons along the way. Matt shares what he’s learned about what he calls our most ‘misunderstood’ ally. The stories and songs are about: Why do French people not get fat? Are they rude? And do they hate Americans? He talks, and sings about these things in a wonderfully humorous way. You get caught up in the stories and then realize not only is Matt a great story teller, but he has a really strong voice. He generally stays away from politics in the show but does suggest he left the United States when George W. Bush became president, and returned when Obama was elected. He didn’t actually say what he wants to do today, but the audience did get the idea.
After living in Paris, he came back to the U.S. and had what he calls, ‘a second awakening.’ He worked with a vocal coach, met and became friends with many in the theater world and did his first show, “A Pleasure to Have in Class,” which is stories and songs about his life as a people-pleaser, from childhood to his gay divorce. This second show he shared with the public for the first time in 2023 at The Green Room 42.
Matt told Broadway World, “to do a one-man show, you first have to have the confidence you have a story to tell, that you have something to share with people. Not just something that you want to say, but something relatable that will connect with the audience. And then you have to work with a good team. You need a director that can help you shape an arc out of the story and make sure that it’s not just therapy on stage. So having a good team, making the right musical choices, making sure that you’re not coming from too self-centered of a place, has been key for me.” Matt followed all that advice well, and the result is the wonderful “Make Me French.”
This is the first show Matt has done outside of New York. I hope for audiences it won’t be the last. The world awaits this talented performer. You can follow Matt on Instagram and on his website, showtunesmatt.com. The Clear Space cabaret series continues all summer; visit clearspacetheatre.org for tickets.
Now the disclaimer: I am not related to Matthew Rosenstein, and this is an unbiased review. It would be nice to be related to such a talented guy, but we have found no indication we share any relatives at all. I first met Matthew after his show at Clear Space Theatre in Rehoboth Beach.
Peter Rosenstein is a longtime LGBTQ rights and Democratic Party activist.
Germany
We must not scapegoat refugees after Berlin Pride terrorist attack
‘LGBTI people must not be instrumentalized to spread hatred against others.’

On Saturday, during Berlin’s Christopher Street Day, one of Europe’s biggest LGBTQ Pride events, a 21-year-old religious extremist drove a van into the crowd and then used a knife to stab multiple people. One person died and 29 others were injured.
When I saw this news on social media, I sincerely felt scared, and not because one more bigot used his religion to justify violence against people like me. It has, unfortunately, happened too often. Despite being happy to see the overwhelming support for the queer community and the condemnation of terrorism, I was terrified by the wave of Islamophobic and anti-immigrant statements that came even from “left” and “progressive” people who should know better, who generally support refugees, who know that all people are equal, and that you shouldn’t treat others as less human because of their religion.
In 2020, a Russian MP threatened to start a criminal case against me after I interviewed Muslim women about why they called themselves feminists and wrote about my own relationship with feminism and Islam, mentioning that I was following events in Syria and had read some academic books on the Islamic State. Surprisingly, the MP claimed that I was recruiting women to ISIS by using feminist ideas, which, of course, was absolutely ridiculous for many reasons, including the fact that I was an openly nonbinary transgender person. But some media outlets and queer people online, including those who called themselves progressive, refused to support me or believed the lie. This is what an anti-extremist witchhunt looks like. If I had been in Russia, and not in the UK, I probably would have been in prison.
It is extremely important to oppose extremism by knowing the actual facts about terrorist groups and not starting a moral panic.
Here are four examples of what media coverage and queer people online often misunderstand about the events in Berlin, and why it’s important.
1. Islam is not the problem
Despite a common misunderstanding, this terrorist act wasn’t even about Islam.
Islam, just like Christianity and Judaism, has a variety of views on LGBTQ rights, from affirmative to condemning. I think everyone in the American Bible Belt has met Christian fundamentalists who praised violence against LGBTQ people or used violence against their own queer children, so it is a universal problem. But the thing is Abdul Ballout was not an ordinary conservative Muslim. He was known for wanting to join ISIS. It is an apocalyptic cult that teaches that we are living in the last era, so they are trying to re-create the caliphate that they believe should be restored before Doomsday.
Most of the Muslim people I know, including conservative Salafi Muslims, see the group as dangerous criminals, or don’t see the group as a Muslim group at all. The vast majority of ISIS victims are not Western people or queer people, but cisgender heterosexual Muslims in the Middle East and Africa who the group considers to be infidels. ISIS is widely condemned by Muslim communities and scholars, and blaming Islam for the actions of cult members is like blaming Christianity and all Christians — or even all Christian fundamentalists — for the actions of Branch Davidians members or for the mass murder-suicide committed by members of the People’s Temple.
2. Refugees are not the problem — and Germany is not a safe haven for refugees
First, the attacker was a German citizen. But the media continue to blame migration. Germany is seen as a safe haven for refugees and asylum seekers in the U.S., the UK and beyond. But the time when Germany was safe is long gone. For refugees from Russia between 2022 and 2025 alone, around 90 percent of refugee claims have been refused by Germany, including the claims of political prisoners. The situation for non-White Muslim refugees is even worse, especially in regions such as Bavaria.
I have personal experience working with some refugees in Germany who are also Muslim. The way the migration service mistreated them is beyond anything I saw while working with refugees and being a refugee in the UK. I saw cases in Germany where an asylum seeker’s family was threatened back home because of social media posts the asylum seeker had made, or where a person was detained and sent back to their homeland despite having a history of persecution and torture by the government. Very often, when a person is taken by the immigration service, their loved ones don’t know where they are. Queer refugees also report homophobic and transphobic attitudes in the system.
The narrative that Germany is too generous to refugees was created by the far right and has little to do with reality, and it harms actual refugees, including queer refugees, by silencing their voices.
3. There is no collective responsibility
It is an extremely old and dangerous idea.
Just as all gay men shouldn’t be blamed for what the American serial killer Jeffrey Dahmer did just because he was gay; we shouldn’t blame all Muslims, all people of Middle Eastern origin, or any other large demographic group for the crime of one terrorist. Even if the terrorist had been a refugee and a Muslim, it shouldn’t actually matter, because under the law in any modern non-authoritarian country, an individual shouldn’t be held responsible for the actions of their social group.
After all, when a white, Christian, cisgender, heterosexual, neurotypical person commits a crime, it is almost always seen as an individual’s fault. Why is it different for marginalized groups? The idea of collective responsibility harmed the gay community for decades and is harming the trans community right now, for example after Charlie Kirk’s murder. The best thing we can do is stop this narrative, because it will be used against us.
The only reason I explained about ISIS and the refugee experience in Germany is to show how far from reality the popular accusations are.
4. Witch-hunts and scapegoating serve the far-right agenda and are extremely anti-queer
From my own experience, as an openly trans person speaking against Islamophobia, sexism and queerphobia who was accused of supporting the cult that kills queer people, promotes the sexual exploitation of women and sees the majority of Muslims as legitimate targets, I can say for sure that moral panic can go wild.
People who remember the Satanic Panic of the 1980s, or even the attacks on Muslim communities after Sept. 11, should know this.
Now even queer people are attacking refugees and Muslim communities online while the German government is introducing more draconian measures against those groups.
ILGA-Europe, the biggest LGBTQ organization in Europe, made a statement warning against any attempt to weaponize the attack.
“This tragedy must not be used to fuel hatred against migrants, foreigners or Muslim communities. We reject any attempt by anti-democratic actors to exploit what happened to divide communities, scapegoat minorities or turn one group against another,” Chaber, the group’s executive director, said. “LGBTI people must not be instrumentalized to spread hatred against others, nor should the existence of racism, Islamophobia or anti-migrant hatred be used to minimize the threats faced by LGBTI people. The rights, safety, and dignity of all people must be defended.”
People who live at the intersection of multiple marginalized identities — LGBTQ Muslims, LGBTQ people of color and LGBTQ refugees — will probably suffer the most from this moral panic. Moreover, these are the same political groups that target refugees, Muslim communities and queer people. If this hatred isn’t stopped now, everyone is potentially at risk.
Condemning terrorism is important, but it is no less important to stop creating more victims.
Opinions
Pentagon says hormones make trans troops unfit but gives them to men
A man who needs a screening program to feel like a warrior is telling on himself

Last week, the Secretary of Defense posted a video to announce what he called the “High-T Department of War.” In it, Pete Hegseth ordered annual testosterone screening for every service member over 30 and offered testosterone therapy to those who want it, all in the name of keeping American warriors, in his words, on the “leading edge of lethality.” A hormone, he explained, is part of “the biological foundation required to sustain the fight.”
I have spent years writing about masculinity, so I know a performance when I see one. But this one is different, because at the exact moment Hegseth is prescribing testosterone to the men, his department is throwing other Americans out of uniform for taking it.
Here is the contradiction, and I promise I am not the one straining to find it. Since early 2025, the administration has worked to remove transgender troops from the military. One of its stated reasons, laid out in the executive order and in the government’s own court filings, is that these service members require ongoing medical treatment the military cannot easily sustain. Hormone therapy, the argument goes, means cost, monitoring, lab work, and stretches of non-deployability. A soldier who needs a standing prescription, the logic runs, is a burden the force cannot carry.
Then the same department launched a program to put a standing hormone prescription in the pocket of any man over 30 who wants one.
You do not have to take my word for the hypocrisy. A federal judge has already put it on the record. Last Wednesday, in the case challenging the transgender ban, Judge Ana Reyes took formal notice of the new testosterone program and ordered the government to explain how the very same class of treatment can be readiness-enhancing for one group of troops and disqualifying for another. It is the question at the center of the case now. Reyes has been skeptical of the medical argument from the start. Last year she pointed out that the military spent roughly $41 million on Viagra in a single year, and called transgender care, by comparison, “not even a rounding error.”
That is the tell. It was never really about the medicine. Testosterone is testosterone. The prescriptions, the monitoring, the lab work, the deployability questions are identical whether the person filling the vial is a trans man or a cisgender colonel chasing his youth. The only thing that changes is who is holding it. When the man taking the hormone fits the picture of a warrior, the treatment becomes “lethality.” When the man taking it is transgender, the identical treatment becomes a fatal risk to readiness. The medicine did not change. The identity did.
I want to be fair, because the argument only works if it is honest. The government has other claims in the case that a court has not yet resolved, about surgeries, about facilities, about unit cohesion, and it insists that cisgender men on testosterone and transgender men are simply “not similarly situated.” Those arguments can be debated on their merits. But the medical one, the claim that hormone therapy itself is too much for the military to manage, is the one Hegseth’s own policy just detonated. You cannot brand testosterone a warrior’s birthright on Monday and a disqualifying liability on Tuesday and expect a judge, or the rest of us, not to notice.
And notice what the whole spectacle is actually selling. A “Department of War” rebrand. A hormone reframed as a weapon. A Secretary who mocks “dudes in dresses” while rolling out mandatory bloodwork so the men can optimize their manhood by the milligram. This is not a medical policy. It is a theory of masculinity, the same tired one, that a man is a number on a lab report and a posture for the camera. It arrives, not coincidentally, as the administration moves to loosen testosterone prescribing across the country, turning manhood into a supplement you can top off.
I have known a lot of strong men. My father crossed an ocean as a laborer to build a life; the strongest men I was raised by never once measured themselves in a vial. Real strength was never a hormone level, and the men who most need to announce their lethality are, with remarkable consistency, the ones least sure of it.
The House declined last week to write the transgender ban into law, so it still rests on nothing sturdier than executive will and a medical excuse. That excuse just ran out of testosterone. A man who needs a screening program and a war-department rebrand to feel like a warrior is telling on himself. The rest of us should say so out loud.
Dimitrios Aletras is a queer, first-generation Greek-American writer and survivor-advocate, with work published in Salon, The Advocate, and the Reading Eagle.

Madonna to perform at World Pride in Amsterdam

‘Heartstopper Forever’ delivers satisfying conclusion

Matthew Rosenstein in ‘Make Me French’ a hit at Clear Space Theatre

White House orders warning signs at Smithsonian over gender identity exhibits

Rainbows in Revolt on a mission to make LGBTQ artists’ voices heard

1 dead, 29 injured in Berlin Pride attack

‘Into the Grey’ unites Cavill, Gyllenhaal for thrills and gay love

D.C. summer theater offers something for every taste

Summer in the City: Free exhibits, movies, more fill D.C.’s calendar

With gas prices soaring again, a staycation is a good plan
-

 Germany4 days ago
Germany4 days ago1 dead, 29 injured in Berlin Pride attack
-
Movies5 days ago
‘Into the Grey’ unites Cavill, Gyllenhaal for thrills and gay love
-
Theater3 days ago
D.C. summer theater offers something for every taste
-
a&e features3 days ago
Summer in the City: Free exhibits, movies, more fill D.C.’s calendar