National
In Congress: Many bills, but no timetable for progress
Pro-LGBT legislation stalls as November elections loom

Congress could be poised to pass several pro-LGBT bills in the months that remain in this year’s legislative calendar, although Capitol Hill observers say the schedule for when the bills would see votes remains unclear.
In the wake of successful votes late last month to repeal “Don’t Ask, Don’t Tell,” Congress could see momentum to pass other major legislation, such as the Domestic Partnership Benefits & Obligations Act and the Employment Non-Discrimination Act.
Rep. Tammy Baldwin (D-Wis.) said in an interview with the Blade this week that she had renewed optimism about the domestic partner benefits bill, which she sponsors in the House.
“One issue that got renewed momentum over this Memorial Day recess was my bill to provide domestic partnership and obligations to federal employees and their partners,” she said.
Baldwin, the only out lesbian in Congress, said the issue received additional attention last week when President Obama enacted limited partner benefits for federal employees through administrative action.
“At the same time as he signed this presidential memorandum, he called on the Congress to send [my bill] to his desk because he can’t provide some of these very important benefits like health insurance and certain pension benefits without our passing legislation,” Baldwin said.
In a statement commending Obama for issuing the benefits, U.S. House Speaker Nancy Pelosi also spoke favorably about the Domestic Partnership Benefits & Obligations Act as one way to offer additional benefits to federal workers.
“Congresswoman Baldwin’s bill will continue to move forward in the House and we look forward to its progress in the Senate,” Pelosi said.
The domestic partner bill had significant momentum late last year when House and Senate committees reported it to the floor in each chamber. For a time, the legislation had stalled due to cost offset questions, but congressional leaders have said they’ve since received the necessary information.
Baldwin said staffers of the House and Senate leaders on the legislation met Monday to discuss the bill’s path, and lawmakers in both chambers are ready to move forward.
In a statement to the Blade, Sen. Joseph Lieberman (I-Conn.), the sponsor of the bill in the Senate, said the bill would be ready for floor consideration “within weeks.” Lieberman noted this estimate was for when the bill would be ready to go to the floor, not when a vote would occur, and that Senate Majority Leader Harry Reid (D-Nev.) is “responsible for setting a timetable for consideration of legislation.”
Jim Manley, a Reid spokesperson, said a vote hasn’t yet been scheduled.
Baldwin said she couldn’t offer a more specific timetable for when she expects the legislation to advance.
“A lot happened over the course of this recess in terms of adding momentum for the legislation,” she said. “Because it happened over the recess, and I’ve been in Wisconsin, and not in Washington, and not able to have conversations with my leadership and with the other players in this, I can’t tell you if there’s a timetable yet.”
Allison Herwitt, legislative director for the Human Rights Campaign, also said she doesn’t know when Congress would bring the measure to the floor for consideration.
“Again, the question is how to move forward and what’s the timeframe for moving it forward, so we continue, as we have been for the past year, advocating to get this bill done,” she said.
ENDA faces obstacles
LGBT rights supporters have also strongly pushed for Congress to take up ENDA, which would bar employment discrimination against LGBT people in most public and private workplace settings.
The legislation remains pending in House and Senate committees. Capitol Hill observers have said ENDA supporters lack the 60 votes to overcome a filibuster in the Senate.
Still, supporters have expressed optimism about moving forward with the bill in the House. Baldwin said the LGBT Equality Caucus has been “counting the votes” and asking lawmakers how they would vote on the legislation or a harmful motion to recommit on the measure.
“It’s looking strong,” Baldwin said. “I’m hopeful that we can see committee consideration and floor passage very shortly.”
Rep. Barney Frank, who’s sponsoring the bill in the House, has told media outlets that a vote could take place this month or next.
But a more specific time for when Congress might take up ENDA is unclear. Aaron Albright, a spokesperson for the Education & Labor Committee, said he didn’t have an update or estimate on the schedule for committee action on the legislation.
Baldwin said her “crystal ball has been very unclear” for ENDA consideration and that she couldn’t offer a more definite timeframe.
“I was hoping it would be some months ago, but we continue to go through the vote counts, try to make sure they’re as solid as possible,” she said.
Herwitt was similarly unsure about when ENDA would come to the House floor, although she said HRC was pushing for it to come before lawmakers.
“Obviously, HRC wants a committee markup and a floor vote as soon as possible,” she said. “We would like to continue the momentum on moving LGBT equality forward and we would like a House vote as soon as possible.”
One danger for ENDA in the House is a legislative maneuver known as the motion to recommit, which could derail the legislation once it comes to the floor. A successful vote on the maneuver on the floor would enable opponents to send the motion back to committee.
Supporters have said opponents could target the bill’s gender identity provisions in the motion to recommit, although what’s targeted wouldn’t necessarily be such language.
Baldwin said “there are a lot of meddlesome things” that ENDA’s opponents can do through a motion to recommit when the bill comes to the floor.
“So we have been really trying to ask colleagues how they would vote in a wide variety of scenarios, so that we can feel confident that we have the votes to defeat such a motion to recommit,” she said.
Herwitt noted there’s “still some concern” and “vote counting” happening around the motion to recommit.
“We remain concerned to the extent that we want to continue working with leadership to shore up the votes that we need, so that when the bill comes to the floor, we have the ability to beat back a motion to recommit,” Herwitt said.
Herwitt said Pelosi has expressed a commitment to move ENDA to the floor, but wants to “make sure that we’re looking at angles in terms of what the motion to recommit would be, to protect the integrity of the bill.”
“If she brings the bill to the floor, she doesn’t want to lose,” Herwitt said. “So, she’s an expert vote-counter. She was a whip for many years, and so she knows what it takes to get a bill to the floor. From everything I’ve heard from her people, she wants to get it done, but she wants to get it done right.”
Another pro-LGBT bill pending before Congress is legislation that would enable same-sex bi-national couples to remain together in the U.S.
Current immigration law prohibits LGBT Americans from sponsoring their foreign partners for residency in the United States. Consequently, some LGBT Americans are faced with losing their partners after visas expire, while others expatriate with their partners to other countries with more favorable immigration laws.
Standalone legislation known as the Uniting American Families Act would rectify this situation. But supporters of the measure see its inclusion as part of upcoming immigration reform as the optimal path for passage.
Heading the legislative effort for comprehensive immigration reform in the Senate is Sen. Chuck Schumer (D-N.Y.). His office didn’t respond to a request to comment on the timing for immigration reform or whether UAFA would be included in the legislation.
Still, Schumer has spoken favorably about the inclusion of UAFA in comprehensive immigration reform, and advocates are expecting him to include the provision in the bill once it’s introduced.
According to the news website IrishCentral.com, Schumer said last week at a fundraising event for Irish Lobby for Immigration Reform that he thinks Congress will finish immigration reform by March 2011 — if not by the end of this year.
Steve Ralls, spokesperson for Immigration Equality, said supporters of the legislation have been assured Schumer wants UAFA as part of comprehensive immigration reform.
“I would even say, at this point, that the expectation is that UAFA will be part of comprehensive reform,” Ralls said. “I think Immigration Equality and other immigrant advocates fully expect it to be an inclusive bill when it’s introduced.”
Still, when Schumer will introduce the legislation in the Senate remains unclear. Since the Senate Judiciary Committee would handle both immigration reform and U.S. Supreme Court nominations, many Capitol Hill observers believe the Senate will first approve the nomination of Elena Kagan to the Supreme Court before taking up the immigration issue.
If Schumer includes UAFA as part of comprehensive immigration reform, the larger bill could find opposition from conservative groups that say they won’t support immigration reform with language benefitting same-sex couples.
Last week, the Liberty Counsel issued a statement signed by other Christian evangelical leaders saying comprehensive immigration reform that includes UAFA would not advance in Congress.
“Same-sex domestic partnerships will doom any effort for bipartisan support of immigration and will cause religious conservatives to withdraw their support,” said Mat Staver, founder and chair of the Liberty Counsel. “If same-sex domestic partnerships are included, the immigration bill will have no chance of passing.”
In response, Ralls said the “cornerstone” of the U.S. immigration system has been family unification and that LGBT families “should be part of that noble commitment.”
“Despite the protests of a few, many people, including many faith communities, continue to support an inclusive immigration reform bill,” Ralls said. “Methodists, Episcopalians, Jewish organizations, Unitarians and others are holding strong to a belief that a truly pro-family bill must include every family.”
Other bills on deck
Other pro-LGBT bills also could come up for consideration by the end of this year.
One bill, known as the Student Non-Discrimination Act, would bar schools from discriminating against LGBT students or ignoring harassing behavior against them. Potential penalties for discrimination could include a loss of federal funding or a legal cause of action for victims.
As standalone versions of the legislation remain pending in the House and Senate, supporters have said they envision passage of the bill as part of the upcoming Elementary & Secondary Education Act reauthorization.
Still, it’s unclear when Congress will take up this major education budget legislation. A House Democratic leadership aide noted the bill hadn’t yet been introduced, and “we can’t determine the timeline until that happens.”
Should Congress begin work on the education bill, Herwitt said HRC would push for the Student Non-Discrimination Act’s inclusion as part of the larger legislation.
“If the ESEA bill moves forward, you will see HRC and other groups like [the Gay, Lesbian & Straight Education Network] working hard on the bill to make every effort to have it be part of the reauthorization bill,” Herwitt said.
Herwitt said she’s heard conflicting stories on the education reauthorization, though, and was unsure time remains in this year’s legislative calendar to tackle the legislation.
Baldwin said the Student Non-Discrimination Act’s “brightest prospect” is inclusion as part of this larger legislation, but she noted if the process stalls, congressional hearings would help educate members of Congress on the importance of the issue.
“One of the things I would really hope for is hearings on that legislation to really educate members and the public on what a significant issue this is,” she said. “I think many are unaware, and I think you could build some real momentum for passage of the legislation if it were highlighted in that way.”
Also of interest to LGBT rights supporters is passage of the fiscal years 2010 and 2011 foreign affairs reauthorization legislation.
Last year, the House approved a version of the State Department budget legislation that would call for greater U.S. action against LGBT abuses abroad. In the Senate, legislation with identical language has been reported out of committee, but hasn’t yet reached the floor.
The language urges the State Department to task more officers in the Human Rights Bureau to track violence overseas related to sexual orientation and laws criminalizing homosexuality.
Additionally, the provision calls on U.S. embassies to work to reform or repeal laws overseas criminalizing homosexuality and directs the State Department to strengthen its annual human rights report with regard to reporting on abuses against LGBT people.
But whether Congress will manage to pass the reauthorization bill for the State Department remains in question. The last time this legislation made its way to president’s desk was in 2002, and Manley said nothing has been scheduled for when the bill would come to the Senate floor.
Mark Bromley, chair of the Council for Global Equality, was skeptical that the full Senate would find time soon to take up the measure.
“I haven’t heard anything about them being able to find floor time for it,” he said. “It doesn’t seem like there’s any momentum in terms of getting it to the floor in the short term.”
Herwitt noted that passage of foreign affairs authorization has often been a difficult task for Congress.
“There have been many years when the State Department authorization bill never made it to the floor just because it becomes a heavy legislative lift — not because of our issues, but because of the bigger issues that are in the bill,” she said.
Baldwin said she was nonetheless optimistic about the bill’s chances this year because both chambers of Congress have moved forward on it.
“I would be hopeful — given that there’s interest now in both houses of Congress — that we can see it through,” she said.






National
White House orders warning signs at Smithsonian over gender identity exhibits
Administration criticizes National Museum of American History

The Trump administration will install temporary warning signs outside the Smithsonian’s National Museum of American History after releasing a report accusing the museum of promoting what it calls “radical” gender ideology and other politically biased content.
According to the Executive Order, “For purposes of policy formulation under EO 14253, this review of the National Museum of American History concludes that NMAH, by the intention and at the direction of current Museum and Smithsonian leadership, has become subject to institutional capture by a radical, activist ideology that is fundamentally opposed to telling the noble, honest story of the great country we know and love.”
Executive Order 14253 refers to what the White House has deemed the “Restoring Truth and Sanity to American History” order. Therefore, the Trump administration has said it will take all available steps to ensure that the issues in the report are addressed and rectified.
Without specifying, the White House has stated that warnings will be posted along NMAH to alert visitors to sections of the museum it has deemed are in violation according to the report.
“The Secretary of the Interior, acting through the Director of the National Park Service (NPS) and in coordination with the Assistant to the President for Domestic Policy, shall install temporary signage along the NPS-maintained sidewalks and walkways used by the public to access the Museum, informing visitors of the findings of the Report and of the policy set forth in section 1 of this order,” the Executive Order states.
The warnings were raised in a 162-page report issued by the Domestic Policy Council. The report detailed ways in which the National Museum of American History (NMAH) has “poorly” portrayed American history and insufficiently highlighted the founding story during America 250th celebrations.
The report outlined key findings of the NMAH. One of these findings was the Center for Restorative History within the museum, which has stated its purpose is to “encourage systemic change” by highlighting diverse groups. However, the report states that it highlights every group of Americans except for straight and white Americans.
The Domestic Policy Council accused the museum of engaging in “transgender activism.” According to the report, examples include referring to “biological men” as women or girls, displaying what it describes as sexually suggestive content, and incorporating discussions of gender fluidity, gender identity, and gender nonconformity into the museum’s educational curriculum, “Becoming US.”
The report also criticizes the curriculum for using the term “transgender” when discussing gender-nonconforming people and encouraging individuals to ask a person’s pronouns when meeting them. It further objects to exhibits stating that “transgender, nonbinary, and cisgender female athletes” continue to struggle for and demand equality.
It also condemns what it refers to as explicit content in an exhibition, “Girlhood (It’s Complicated)”, such as chest binders, questioning gender testing in women’s sports, and referring to biological females as “people inhabiting female bodies.”
Additionally, the report accuses the museum of no longer participating in flag-celebrating ceremonies because it was “too busy” preparing for June Pride and WorldPride events. It states, “As Director Hartig explained in a June 2024 presentation, all her attention was focused on flying the Smithsonian Pride Alliance’s ‘intersexual pride flag during June’ in 2023 and 2024.”
On July 9, the American Historical Association issued a statement rejecting the report’s findings.
In regard to the report, it states, “Its anonymous authors overlook a central lesson of the nation’s founding: the United States was forged by finding common purpose amid intense divisions, conflicts, and disagreements.” They argue that only “honest history” can tell the true history of the nation.
House Republicans led a subcommittee hearing that questioned Smithsonian Director Hartig extensively. A main focus of the questions was on the exhibits related to gender identity and whether they were appropriate. In the hearing, Rep. Nancy Mace asked: “When was your gender revealed to you, Dr. Hartig?”
In response to questioning, Hartig stated that the institution is nonpartisan and does not push a specific agenda.
Hartig published a two-page statement ahead of her hearing outlining her thoughts on the situation. In the report, she states that the institution is always open to criticism and will continue to look for ways to improve, but she sees the report as misleading.
“I can attest that the report does not fairly characterize the full body of work at this museum. I am familiar with the depth and breadth of our collections, exhibits, and programming. And while I recognize there is always room for improvement, I also know the beauty, inspiration, and expertise that exists in our museum,” Hartig wrote.
Democrats created their own 16-page report as a rebuttal to the Domestic Policy Council’s report. It argued that the attacks by the current Trump administration are another example of its attempt to rewrite history. Additionally, the report states that no policy changes were included in the Executive Order, as that is beyond the President’s role. “The Report recommends nothing. That is no accident. To recommend an action, the Report would need to identify who is legally empowered to take it, and its own opening chapter concedes the President’s only power is to ‘urge’,” House Democrats wrote.
It is still unclear when the temporary warnings will be installed or what form they will take beyond the requirements outlined in the executive order.
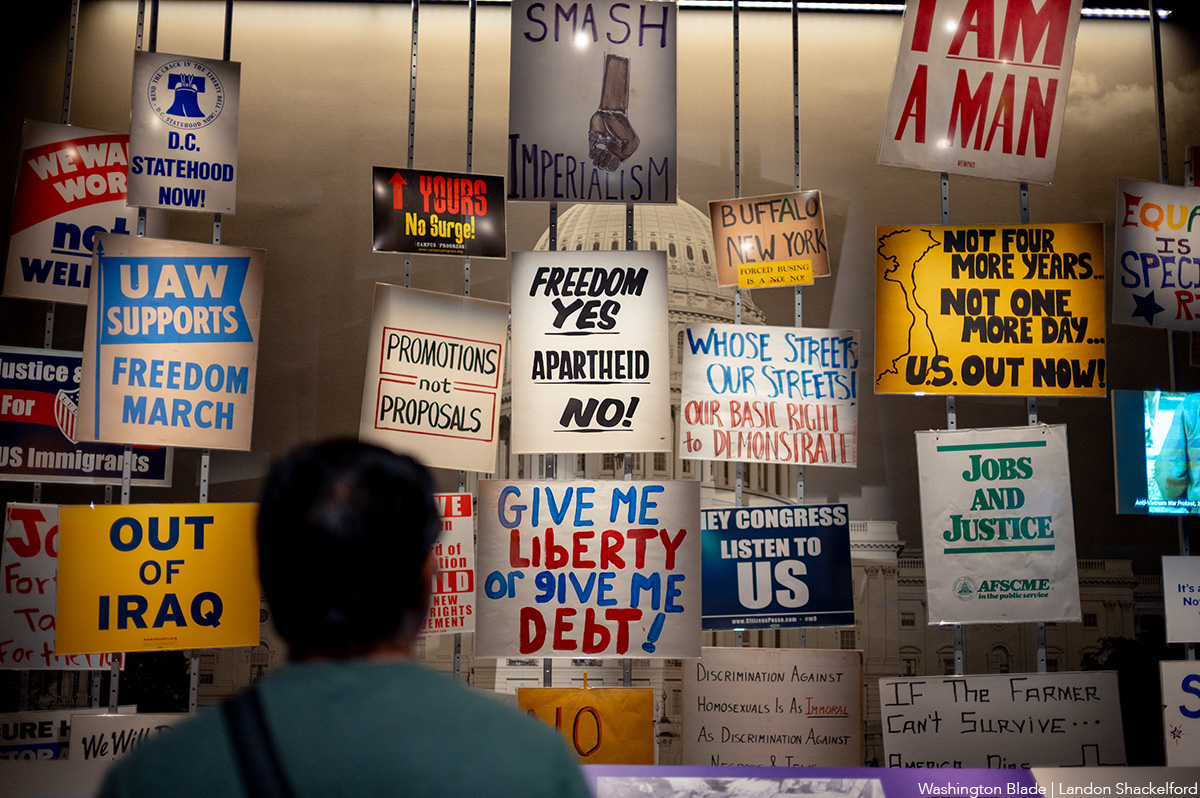
An exhibit at the Smithsonian. (Washington Blade photo by Landon Shackelford)
National
Trump ends direct HIV prevention funding to community groups
Advocates say transfer of funds to states may disrupt local programs

A decision by the U.S. Office of Management and Budget (OMB) at the request of the Trump administration to discontinue direct federal funding of community-based organizations and clinics that provide HIV prevention services has raised concern among community health advocates, including LGBTQ advocates.
News surfaced earlier this month that the OMB informed the U.S. Centers for Disease Control and Prevention that it would not renew $46 million in funding for 96 community-based organizations that provide HIV testing, referrals to medical care, and arrangements for obtaining pre-exposure HIV prevention medication known as PrEP that has been shown to be 99 percent effective in preventing HIV infection.
Under the new policy arranged by OMB, the funds will be redirected to the states to be allocated to state and local health departments. The policy calls for states to encourage but not require their respective state and local health departments to allocate some of those funds for community-based organizations. Under the new policy, the funding is scheduled to last until May of 2027, before a renewal decision is made.
Some political observers have speculated that the decision to end direct federal funding to community-based organizations could be motivated by the Trump administration’s hostility to diversity, equity, and inclusion or DEI programs and organizations that promote those programs, with the belief that some of the groups receiving the federal HIV prevention funds are promoting DEI.
Carl Schmid, executive director of the D.C.-based HIV+ Hepatitis Policy Institute, is among the leaders of many AIDS advocacy organizations expressing strong opposition to the OMB action. Schmid said that in places like D.C. and some states, local officials will be willing to redirect the federal funds to local community-based organizations.
A list of the 96 community-based organizations across the country that are currently receiving the federal AIDS funds includes the D.C.-based Whitman-Walker Health, which has a long history of healthcare support for the LGBTQ community, and La Clinica del Pueblo, which reaches out to the Latino community.
Schmid said Whitman-Walker and La Clinica del Pueblo have longstanding good relationships with the local D.C. government.
“But other states and jurisdictions don’t have that relationship with the community-based organizations,” Schmid said. “It depends on the state,” he said, adding, “Not all states send their money to the communities that really need it most. And not all states are fast in getting money to the community-based organizations.”
Spokespersons for Whitman-Walker and La Clinica del Pueblo couldn’t immediately be reached for comment on whether they think the Trump administration’s latest action related to funding will adversely impact their respective organizations.
Schmid said under the current federal grant program slated to be discontinued, which has been in effect for at least five years, HIV-related health organizations receiving the federal grant funds were eligible for an existing federal policy enabling them to purchase HIV-related medication, including the PrEP prevention medication, at a significant discount from pharmaceutical companies. With the ending of the direct federal HIV funds to community-based organizations, Schmid said it was unclear whether problems may surface in obtaining drug discounts.
“They could still qualify as a sub-grantee from a state,” Schmid said. “But what if they don’t get that grant again? They would not be able to qualify to obtain the drugs” at the discounted price, he said.
Among the organizations expressing strong concern over the decision to discontinue the direct HIV prevention funding to community-based organizations has been the Federal AIDS Policy Institute and its subgroup called the HIV Prevention Action Coalition.
In a July 22 letter bearing the names of 71 community-based organizations from throughout the country sent to U.S. Department of Health and Human Services Secretary Robert F. Kennedy Jr. and Centers for Disease Control and Prevention Acting Director Jay Bhattacharya, the group called for the Trump administration to “reconsider” ending the current funding policy.
“Ending this program without a clear plan for what comes next would dismantle prevention infrastructure that has taken more than three decades of federal investment to build and do so just as that long record of measurable returns is accelerating,” the letter states.
It says the initiative by President Trump in his first term as president to end the HIV epidemic and reduce new HIV infections by 90 percent by 2030 was moving ahead by the funding program for community-based organizations that the administration now wants to end.
“Discontinuing this program would also cost far more than it saves,” the letter says. “Every HIV transmission prevented avoids an estimated lifetime treatment cost of roughly half a million dollars per person to the healthcare system – costs that fall heavily on taxpayer-funded programs, including Medicaid, Medicare, and the Ryan White HIV/AIDS program,” the letter continues.
“The choice before the administration is straightforward: a modest, targeted investment in prevention now, or far greater public expense for treatment later,” the letter concludes.
Spokespersons for the OMB and the Department of Health and Human Services, which oversees the CDC, have not immediately responded to news media requests for comment on the opposition to the funding change policy.
National
At Alliance Defending Freedom’s summit, church and state are one
House Speaker Mike Johnson (R-La.) among speakers

Uncloseted Media published this article on July 23.
By SPENCER MACNAUGHTON | Earlier this month, hundreds of people filled a conference room in San Diego. These included Speaker of the House Mike Johnson, Assistant Secretary of Health Admiral Brian Christine, OpenAI executive Dean Ball, and the attorneys general of West Virginia and Idaho.
They all came together for Alliance Defending Freedom’s 2026 Summit. The Christian legal group, also a Southern Poverty Law Center-designated anti-LGBTQ hate group, described the event as a “gathering of leaders from many different spheres, including law, public policy, media, business, education, and Christian leadership.”
Johnson — who has said that “homosexual relationships are inherently unnatural and … society cannot give its stamp of approval to such a dangerous lifestyle” — was a featured speaker.
In his speech, he seemed unconcerned with the separation of church and state: “It is so encouraging to Kelly and I to be among friends and fellow warriors for this cause and people who understand that God is not done with America yet. … ADF’s on the very tip of the spear, front line, defending those very truths and keeping the door open for the spread of the Gospel. This is our moment. I’m telling you, I believe the next season … is going to be the greatest season of this ministry since its inception.”
That ministry is one that has espoused aggressively anti-LGBTQ views since its inception in the early 1990s. It was co-founded by a group of evangelical men, including Alan Sears, who co-authored a book called “The Homosexual Agenda: Exposing the Principal Threat to Religious Freedom Today.” Since then, ADF has opposed gay marriage and supported bans on gay sex and on gender-affirming care for minors.
After helping overturn Roe v. Wade, ADF lawyers have led key victories at the Supreme Court. In 303 Creative v. Elenis, SCOTUS ruled that a website designer could refuse service to gay weddings. And this year they convinced the Court to overturn Colorado’s ban on conversion therapy and to uphold state laws in West Virginia and Idaho that ban trans girls from playing on girls’ sports teams.
At the summit, ADF President Kristen Waggoner, who has promoted conversion therapists and consistently misgenders trans people, interviewed these states’ attorneys general.
“The lawyers who were defending women’s sports were among the best I’ve ever seen in my entire life,” West Virginia Attorney General JB McCuskey told Waggoner.
Similar to Johnson, Trump’s Assistant Secretary of Health Christine showed his commitment to governing based on conservative Christianity. He gave a Bible-thumping speech against gender transition and trans healthcare, saying that it “contradicts … the deeper moral order that is woven into creation itself. For Genesis 1:27 informs us that God created man in his own image. … Male and female” He also said the “complementary relationship between man and woman is divine” and advocated for youth with gender dysphoria to receive care from a pastor.
All of these remarks from politicians made me think of the interview I published earlier this week with Pete Hegseth’s pastor, Doug Wilson. He wants a Christian theocracy in America and told me that: both the perpetrator and the victim should be disciplined in some cases of marital rape; that transgender people are “sad;” that execution is justifiable for certain homosexual acts; and that gay sex should be illegal.
The ADF Summit is glossy and polished. And while its messaging may be less explicit than Pastor Wilson’s, the track record of the organizations shows they have the exact same desires. They’re just deeply strategic in what they say and when and how they say it.
I believe the political power players who attended this year’s summit know this. They know they are endorsing an organization whose members have essentially called for the illegalization of most — if not all ‚ forms of queer behavior and presentation.
In the last few years, these perspectives have become increasingly embedded in the highest rooms of the federal government and they have been effective in stripping away LGBTQ rights. Wilson, who just installed a full-time pastor in Washington to lead services, says there are 10 to 20 government officials who align with his church’s ideology.
It is vital for Americans to keep their eyes wide open to the ultimate goal of groups like ADF: to create a United States that leaves LGBTQ people without rights and that pushes us back in the closet.

My evening with Madonna

PHOTOS: Petal Release Party

Madonna headlines World Pride Music Festival in Amsterdam

Reggie White relishing first season as artistic director of Woolly Mammoth

PHOTOS: Amsterdam Pride Canal Parade

PHOTOS: Lambda Legal in the Pines

Calendar: July 31-August 6

Taiwan’s government has failed to update process to change gender markers on ID documents

Come showcase your singing, poetry talent