National
Latter-day doubts?
Local LDS member recalls suicide attempt, but remains in Mormon church

Michael_Key")
‘I felt like I had to choose which half of me had to die,’ said David Baker, a local gay Mormon who attempted suicide in 2008. (Blade photo by Michael Key)
David Baker is living what he calls the “ultimate paradox.”
Like many 21-year-old gays in the D.C. area, Baker spent last Saturday at Town as he does many weekends. A drag show is taking place downstairs, but he and his friends went to the upper level to dance to the latest remixes.
“I started going clubbing shortly after I came out,” he said. “But I don’t go all that regularly — probably once a month.”
But on Sunday, the situation is different. After donning his best church clothes, the Salt Lake City native who now lives in Rockville, went to a Mormon church in D.C. for a three-hour block of weekly service.
Activities included hearing speakers from within and outside the congregation and scripture discussion. Baker, a University of Utah graduate, is also co-chair of the cultural events committee and helped work to plan social events with other church members.
Baker’s presence among his congregation is distinct because he’s openly gay in a religion known for its hostility to homosexuality and opposition to same-sex marriage. The Mormon Church earned scorn from many in the LGBT community in 2008 for taking a lead role in backing Proposition 8 in California, which ended same-sex marriage there.
“It’s the ultimate paradox,” Baker said. “It’s been a struggle not just in dealing with my sexuality, but in the reactions that I get from church members sometimes or the reactions that I get from the gay community.”
Even though he stands out for being gay, Baker said he’s able to mingle with other churchgoers and voice his opinion that he’s the same as any other Mormon despite his sexual orientation.
“Lots of people tune me out, but I try and approach it from a concept that we are all children of God, that we are sinners and we are all imperfect,” he said. “So to judge one sin as being worse than others, and my quote-unquote sin being worse than yours is absurd. And that seems to be a message that people understand.”
His path to personal acceptance hasn’t been easy. Baker once considered seeking out shock therapy to alter his sexual orientation as well as participation in Evergreen, the Mormon Church’s reparative therapy program. Such programs were long ago discredited and repudiated by medical professionals.
“I had come out to my family and a couple of friends and it wasn’t so much, ‘Oh, dang it, I’m gay,’ it was, “OK, I’m gay. I accept it. How does this comport with my faith?” he said. “So, I spent pretty much just every waking hour just poring over scripture, poring over words of prophets, poring over everything I could find on sexuality and religion.”
In 2008, Baker attempted to commit suicide by taking an overdose of pills. His roommate found him and took him to a local hospital for treatment.
“I felt like I had to choose which half of me had to die,” he said. “And I got to the point that I thought if half of me has to die, and I still won’t know the truth, why not just kill all of me and then I can finally know the truth?”
While undergoing treatment, Baker said a psychologist suggested to him there could be a distinction between the word of God and the guidance of the church. His roommate came to visit him and made the same observation in the exact same words.
“It sort of caught in my mind that maybe there’s a distinction between what God is saying and what the Prophets and the Apostles are saying,” he said. “Maybe these leaders of the church are Mormon and everything they say is not a direct fact from God, but instead tinged with their own personal beliefs, however flawed they might be.”
Baker is one of many other gay Mormons in the D.C. area who continue to practice their faith despite the religion’s position on homosexuality.
About 60 Mormons or former Mormons are affiliated with the D.C. chapter of Affirmation, a group for LGBT members of the Church of Jesus Christ of Latter-day Saints.
Fred Bowers, Affirmation’s D.C. chapter leader, said about one-third of those on his organization’s mailing list still identify as Mormons and participate in the Mormon church, although to varying degrees.
“Some people may go only to the church on Sunday and some may be more active with other things the church is doing through the week,” Bowers said. “And some may be there active, but they only participate in what they select, but there are a good number that actually do still attend church.”
Those who are Mormon and openly gay face challenges in adhering to their faith. For example, Mormons engaged in same-sex relationships aren’t permitted to attend special services, such as weddings, in Mormon temples. Those who are sexually active in opposite-sex relationships outside of wedlock or those who consume alcohol are similarly unable to attend.
But Bowers said many LGBT Mormons stick with their faith simply because they truly believe in the church’s teachings or because their families have a long history with the religion.
“They’ve grown up with this.” Bowers said. “Just like an Episcopalian or Catholic or what have you, we still believe that. It hasn’t changed just because we’re gay or lesbian. We still believe in that church and we still believe in the principles of it.”
That’s the situation for Baker, who said he still considers himself a Mormon because he believes in the Gospel as presented by the church and because “they have the most truth.”
“That being said, I don’t think that they have it all,” he said. “One of the core articles of faith of the church sort of says that blatantly. It says that we believe all that God has revealed isn’t all that he’ll reveal, and we believe that he’ll yet reveal many great important things. So it’s very much an ongoing, open canon.”
Still, Baker said he’s adapted Mormon dogma into his own views of his sexual orientation. He said he doesn’t plan to have sex until he finds another man to marry — similar to how many straight Mormons abstain from sex until after they receive their nuptials.
“For me, no sex before marriage means a legal marriage because the church does recognize legal marriages — the traditional kind naturally — that aren’t performed in the temple,” he said. “And so, in my mind, that same non-temple civil ceremony would be recognized by God.
‘Wickedness never was happiness’
The difficulty of being Mormon and openly gay became particularly pronounced last week when a high-ranking leader of the church made anti-gay remarks during the 180th semi-annual general conference in Salt Lake City.
Boyd K. Packer, president of the Quorom of Twelve Apostles, called same-sex attractions “impure and unnatural” and characterized efforts to advance same-sex marriage across the country as attempts to “legalize immorality.” Additionally, he suggested people can change their sexual orientation, which can be overcome through prayer.
“We must understand that any persuasion to enter into any relationship that is not in harmony with the principles of the Gospel must be wrong,” he said. “In the Book of Mormon, we learn that ‘wickedness never was happiness.’”
Packer, who as an apostle is supposed to be delivering words directly from God, made the remarks to a crowd of 20,000 people in attendance and millions more watching the sermon via satellite transmission in churches and homes throughout the world.
For many gay Mormons, the words stung. Baker said he “cringed” as he heard Packer’s remarks and left the room where he and others had been viewing the sermon. He then realized he had to watch the entire remarks so he could respond to them later.
“I went back and watched the whole thing, and as I was listening to his words, I just felt frustration and I was very upset by what he was saying because it went against where the church has gone for the last five or 10 years,” he said.
Bowers said the remarks were particularly unfortunate in the wake of recent suicides of gay teens who took their lives after they were bullied and harassed and were disruptive to the dialogue that Affirmation had been pursuing with lower-level Mormon leaders “to heal the damage that was done by Prop 8.”
“They’re working so hard to get some sense of support and everything that we’re working to do that, and then this statement comes along that’s not very helpful,” Bowers said.
Changes were made to the speech in an online version of the remarks published later in the week. Packer’s reference to inborn “tendencies” was switched “temptations.” A question of “Why would our Heavenly Father do that to anyone?” was removed entirely.
Baker said another noteworthy change was the sermon had been downgraded from the level of revelation to a less stringent guide that Mormon church members would do well to follow.
“Before in the mindset of members of the church, it’s been seen as revelation even though it’s never been explicitly said as such,” Baker said. “To have that downgraded from everyone thinking it’s revelation … to actually, no, it’s just a guide, is really big.”
Kim Farah, an LDS spokesperson, said speakers have the opportunity to make changes to clarify their intent on the Monday following every general conference and the changes made to Packer’s sermon were in line with this practice.
“President Packer has simply clarified his intent,” she said. “As we have said repeatedly, the Church’s position on marriage and family is clear and consistent. It is based on respect and love for all of God’s children.”
Even with the corrections, Packer’s sermon has invoked the ire of the Human Rights Campaign, which pounced on the Mormon leader’s remarks.
Joe Solmonese, HRC’s president, called the sermon “inaccurate” and “dangerous” and said it could lead to more LGBT suicides similar to those that took place in the last month.
“When a faith leader tells gay people that they are a mistake because God would never have made them that way and they don’t deserve love, it sends a very powerful message that violence and/or discrimination against LGBT people is acceptable,” Solmonese said. “It also emotionally devastates those who are LGBT or may be struggling with their sexual orientation or gender identity.”
HRC launched a petition campaign against Packer for his remarks following his sermon. On Tuesday, the organization delivered to Mormon Church headquarters a petition signed by 150,000 people asking the leader to correct his remarks further.
Fred Sainz, HRC’s vice president of communications, said the response to the initiative against Packer is the largest for any petition campaign in the organization’s history.
“I think it was the impact of Elder Packer’s words,” Sainz said. “Any one of those issues would have drawn significant scorn from members of the community and our fair-minded straight allies, but when you lump all of them into one sermon, and it comes from the second-highest ranking official of the Mormon Church, I think it rises to the level where people are going to pay attention and demand change.”
Sainz said HRC is seeking a further correction from the Mormon Church because Packer’s remarks were “factually and scientifically untrue.”
“They’re inaccurate,” he said. “And so, they owe the factual record a revision to reflect what is true.”
Michael Otterson, an LDS spokesperson, responded to HRC’s efforts by saying that while the church disagrees with the organization on many issues, they have some “common ground.” For example, Otterson said the church denounces the acts of bullying that led to numerous gay suicides in the past month.
“We join our voice with others in unreserved condemnation of acts of cruelty or attempts to belittle or mock any group or individual that is different — whether those differences arise from race, religion, mental challenges, social status, sexual orientation or for any other reason,” Otterson said. “Such actions simply have no place in our society.”
Otterson maintained the church believes any sexual activity outside of marriage is wrong and marriage should be exclusive to one man and woman. Still, he said these beliefs “should never, ever be used as justification for unkindness.”
“The church recognizes that those of its members who are attracted to others of the same sex experience deep emotional, social and physical feelings,” he continued. “The church distinguishes between feelings or inclinations on the one hand and behavior on the other. It’s not a sin to have feelings, only in yielding to temptation.”
HRC’s effort to draw attention to Packer’s remarks has earned mixed reviews among some gay Mormons. Bowers said HRC’s efforts at drawing attention to Packer’s remarks has been helpful in moving the church to talk about LGBT Mormons in a more positive way.
“This event was very helpful as they did release a statement,” Bowers said. “We’ll look forward to probably hopefully some more positive statements, such as the one they made about … no one should be bullied for anything. They were in agreement that everyone had a right to be in a safe space.”
But Baker was skeptical about the impact that the 150,000 signatures from outside groups like HRC would have on Mormon leadership because he doubted many of the names were from people within the church.
“I don’t think the HRC campaign is going to be that effective in affecting the church, but I definitely think it is proven effective in galvanizing a lot of people for their cause,” he said.
Baker also said the HRC campaign is energizing the core following of the church and noted new Facebook groups such as “I Love Boyd K. Packer” have emerged suggesting that the LGBT organization is bullying the church.
“I think that there’s going to be a bigger fallout of this from inside the church,” Baker said. “And from a member’s perspective, it’s going to be rally together all the other members and be like, ‘Look these people are attacking us. We’re being persecuted.’”
Sainz maintained HRC’s initiative is “not intended against Mormonism” and said millions of fair-minded Mormons “welcome LGBT people and want to encircle them in love and acceptance.”
“We don’t take exception to the Mormon religion,” Sainz said. “Our issue is with Elder Packer’s sermon and it’s with the Mormon Church hierarchy’s conduct on some of these issues. So that is an important distinction that we make.”
A change in the membership core?
As the public campaign between Packer and HRC plays out, a more under the radar effort has also been taking place with LGBT Mormons seeking change within the church — particularly in the wake of the church’s role in Prop 8.
On Sept. 19, Marlin Jensen, a general authority of the LDS Church, held a meeting in Oakland, Calif., with about 90 Mormons who reportedly voiced their disappointment over the church’s involvement in Prop 8 as well as other positions related to LGBT people.
According to Mormon writer Carol Lynn Pearson, some speakers expressed anger that Prop 8 had given Mormons “a license to hate.”
After listening to the stories, Jensen reportedly arose and through tears said, “I know that never in my life will I experience an hour quite like this one” and “to the full extent of my capacity I say that I am sorry.” Still, he never said during his remarks that he felt the LDS support for Prop 8 was an error.
The meeting itself, in addition to Jensen’s comments, was notable for many in the Mormon faith — particularly in light of the fact that apologies from church leaders are uncommon for any reason.
Baker said he thinks the event is “indicative of more of a change within the membership core.”
“The mindset of the membership just sort of realized that, ‘Wow, the church has been really rallying around Prop 8, which has been going on for two years,’” Baker said. “A lot of people are starting to sit and ask themselves, ‘What am I really supporting here?’”
Bowers also said the meeting reflects how Mormons are becoming more aware of LGBT people in their membership.
“They now know from working with them or seeing them come to church and doing their callings and wanting to do things that Mormons do in the church that we are whole, good people,” Bowers said. “Some of that attitude, I think, has changed very significantly based on the work they’ve being doing out in Oakland.”
Baker said he thinks the meeting that took place in Oakland represents how change within the church and its views on homosexuality could take place over time.
“The way the church is set up is it’s going to be something from the inside that changes it — the membership themselves over time grows to sort of recognize homosexuality more rather than just going from a top-down approach,” he said.
In the meantime, Baker plans to continue attending church service as he looks for the right man to marry while occasionally hitting the clubs on the weekend.
“I believe that they have homosexuality wrong and that over time, that might change,” Baker said. “But in the meantime, I still honestly believe in the church. And they do accept me and they don’t hate me, but it is an interesting razor-thin line to be walking.”





Michigan
Progressives score victory as El-Sayed wins Mich. Senate primary
Democratic newcomer will face Rogers in November

Michigan held its primary on Tuesday, allowing the two major political parties to select their nominees to go head-to-head for the state’s U.S. Senate seat.
NBC News called the Democratic race early, giving the victory to physician Abdul El-Sayed over incumbent U.S. Rep. Haley Stevens (D-Mich.) in an extremely close primary. El-Sayed won 48.5 percent of the primary vote, with Stevens trailing by just one percentage point at 47.5 percent.
Both candidates have campagined on supporting the LGBTQ community through different avenues— for El-Sayed he focused on his past promoting HIV and PrEP funding and research. Stevens focused on her legislative history working to support transgender rights in the state.
This is a major win for progressive Democrats, who have been bearing the brunt of political attacks from President Donald Trump, the Republican Party, and centrist Democrats.
El-Sayed, a former health director in Detroit, ran his campaign largely on making life in the Great Lakes State more affordable amid rising costs. His policies include promoting “Medicare for All,” pushing health policy that targets the regressive efforts of the Trump-Vance administration that rolls back funding for both Women and LGBTQ people, minimizing the growing amount of money in politics, and he was very vocal in his criticism of Stevens for supporting aid to Israel. He was endorsed by two major progressives — U.S. Sen. Bernie Sanders (I-Vt.) and U.S. Rep. Alexandria Ocasio Cortez (D-N.Y.).
Stevens, the four-term congresswoman, is much closer to establishment Democrats on policy than El-Sayed.
During her time in the federal government, she has consistently supported the Equality Act, which would add sexual orientation and gender identity as protected classes under the Civil Rights Act of 1964. She has also emphasized supporting local manufacturing and lowering housing costs in the state.
She was named to Advocates for Trans Equality’s 118th Congressional Champions list for her pro-trans policies and was endorsed by establishment heavy hitters Michigan Gov. Gretchen Whitmer and Senate Minority Leader Chuck Schumer (D-N.Y.).
The contentious race boiled down not only to Michigan affairs but also extended to international conflicts — namely Palestine. (South Africa has filed a case in the International Court of Justice in The Hague that accuses Israel of committing genocide in the Gaza Strip after Oct. 7.) This primary also acted as one of the first major races that pushed back against AIPAC, a lobbying group that works to promote pro-Israel candidates in U.S. elections. The group has been involved in domestic politics since 1954.
AIPAC devoted a massive amount of money to this race.
The Associated Press reported that the pro-Israel lobbying group spent more than $30 million on ads against El-Sayed because of his vocal denunciation of Israel and his continued criticism of its policies towards Palestine.
Michigan has a large Muslim and Arab American population, which could, in part, explain how El-Sayed was able to win.
The Republican side was far less competitive. Former U.S. Rep. Mike Rogers (R-Mich.) ran unopposed and clinched the GOP nomination. He has consistently held anti-LGBTQ positions, going as far as voting multiple times for a federal constitutional amendment to ban same-sex marriage, voting against repealing the military’s “Don’t Ask, Don’t Tell” policy, and supporting efforts to directly target the attempted expansion of Title IX protections to include trans people.
El-Sayed will face off against Rogers in November for Michigan’s Senate seat — one that could have lasting impacts not only on the state’s politics but also on the Republicans’ narrow Senate majority and Trump’s political agenda.
National
White House orders warning signs at Smithsonian over gender identity exhibits
Administration criticizes National Museum of American History

The Trump administration will install temporary warning signs outside the Smithsonian’s National Museum of American History after releasing a report accusing the museum of promoting what it calls “radical” gender ideology and other politically biased content.
According to the Executive Order, “For purposes of policy formulation under EO 14253, this review of the National Museum of American History concludes that NMAH, by the intention and at the direction of current Museum and Smithsonian leadership, has become subject to institutional capture by a radical, activist ideology that is fundamentally opposed to telling the noble, honest story of the great country we know and love.”
Executive Order 14253 refers to what the White House has deemed the “Restoring Truth and Sanity to American History” order. Therefore, the Trump administration has said it will take all available steps to ensure that the issues in the report are addressed and rectified.
Without specifying, the White House has stated that warnings will be posted along NMAH to alert visitors to sections of the museum it has deemed are in violation according to the report.
“The Secretary of the Interior, acting through the Director of the National Park Service (NPS) and in coordination with the Assistant to the President for Domestic Policy, shall install temporary signage along the NPS-maintained sidewalks and walkways used by the public to access the Museum, informing visitors of the findings of the Report and of the policy set forth in section 1 of this order,” the Executive Order states.
The warnings were raised in a 162-page report issued by the Domestic Policy Council. The report detailed ways in which the National Museum of American History (NMAH) has “poorly” portrayed American history and insufficiently highlighted the founding story during America 250th celebrations.
The report outlined key findings of the NMAH. One of these findings was the Center for Restorative History within the museum, which has stated its purpose is to “encourage systemic change” by highlighting diverse groups. However, the report states that it highlights every group of Americans except for straight and white Americans.
The Domestic Policy Council accused the museum of engaging in “transgender activism.” According to the report, examples include referring to “biological men” as women or girls, displaying what it describes as sexually suggestive content, and incorporating discussions of gender fluidity, gender identity, and gender nonconformity into the museum’s educational curriculum, “Becoming US.”
The report also criticizes the curriculum for using the term “transgender” when discussing gender-nonconforming people and encouraging individuals to ask a person’s pronouns when meeting them. It further objects to exhibits stating that “transgender, nonbinary, and cisgender female athletes” continue to struggle for and demand equality.
It also condemns what it refers to as explicit content in an exhibition, “Girlhood (It’s Complicated)”, such as chest binders, questioning gender testing in women’s sports, and referring to biological females as “people inhabiting female bodies.”
Additionally, the report accuses the museum of no longer participating in flag-celebrating ceremonies because it was “too busy” preparing for June Pride and WorldPride events. It states, “As Director Hartig explained in a June 2024 presentation, all her attention was focused on flying the Smithsonian Pride Alliance’s ‘intersexual pride flag during June’ in 2023 and 2024.”
On July 9, the American Historical Association issued a statement rejecting the report’s findings.
In regard to the report, it states, “Its anonymous authors overlook a central lesson of the nation’s founding: the United States was forged by finding common purpose amid intense divisions, conflicts, and disagreements.” They argue that only “honest history” can tell the true history of the nation.
House Republicans led a subcommittee hearing that questioned Smithsonian Director Hartig extensively. A main focus of the questions was on the exhibits related to gender identity and whether they were appropriate. In the hearing, Rep. Nancy Mace asked: “When was your gender revealed to you, Dr. Hartig?”
In response to questioning, Hartig stated that the institution is nonpartisan and does not push a specific agenda.
Hartig published a two-page statement ahead of her hearing outlining her thoughts on the situation. In the report, she states that the institution is always open to criticism and will continue to look for ways to improve, but she sees the report as misleading.
“I can attest that the report does not fairly characterize the full body of work at this museum. I am familiar with the depth and breadth of our collections, exhibits, and programming. And while I recognize there is always room for improvement, I also know the beauty, inspiration, and expertise that exists in our museum,” Hartig wrote.
Democrats created their own 16-page report as a rebuttal to the Domestic Policy Council’s report. It argued that the attacks by the current Trump administration are another example of its attempt to rewrite history. Additionally, the report states that no policy changes were included in the Executive Order, as that is beyond the President’s role. “The Report recommends nothing. That is no accident. To recommend an action, the Report would need to identify who is legally empowered to take it, and its own opening chapter concedes the President’s only power is to ‘urge’,” House Democrats wrote.
It is still unclear when the temporary warnings will be installed or what form they will take beyond the requirements outlined in the executive order.
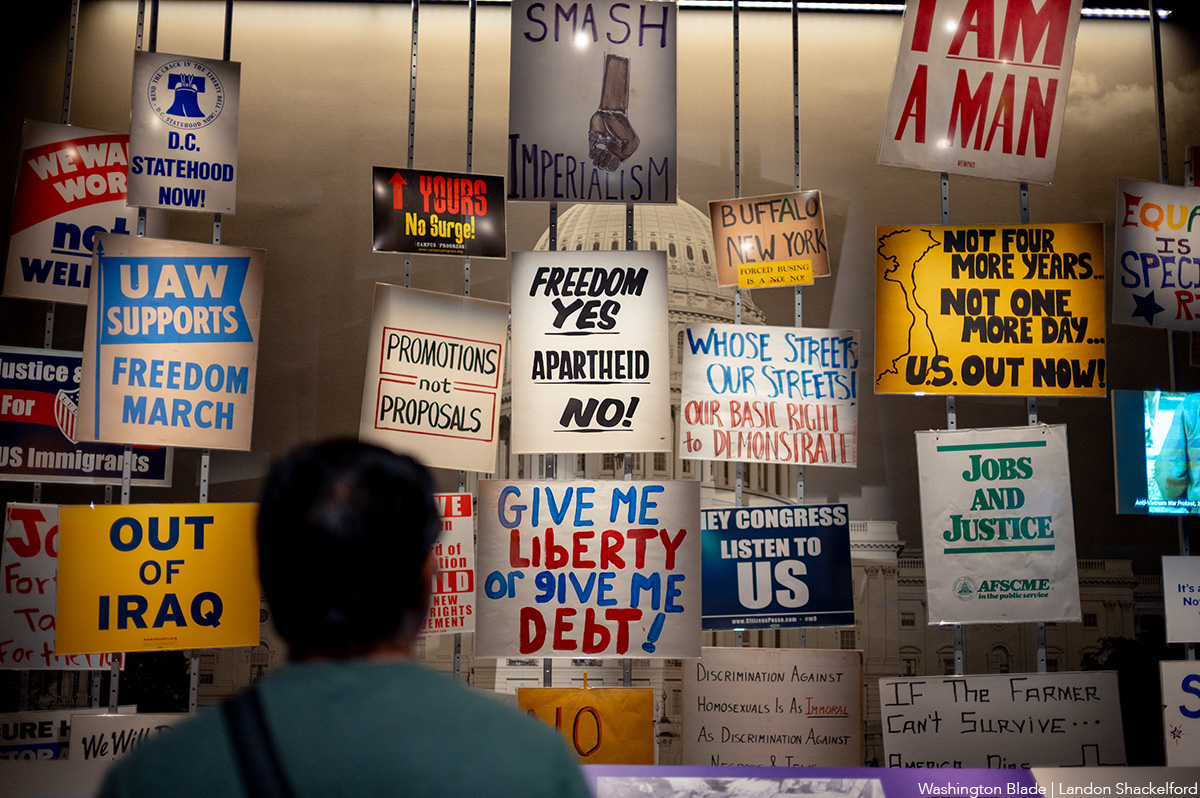
An exhibit at the Smithsonian. (Washington Blade photo by Landon Shackelford)
National
Trump ends direct HIV prevention funding to community groups
Advocates say transfer of funds to states may disrupt local programs

A decision by the U.S. Office of Management and Budget (OMB) at the request of the Trump administration to discontinue direct federal funding of community-based organizations and clinics that provide HIV prevention services has raised concern among community health advocates, including LGBTQ advocates.
News surfaced earlier this month that the OMB informed the U.S. Centers for Disease Control and Prevention that it would not renew $46 million in funding for 96 community-based organizations that provide HIV testing, referrals to medical care, and arrangements for obtaining pre-exposure HIV prevention medication known as PrEP that has been shown to be 99 percent effective in preventing HIV infection.
Under the new policy arranged by OMB, the funds will be redirected to the states to be allocated to state and local health departments. The policy calls for states to encourage but not require their respective state and local health departments to allocate some of those funds for community-based organizations. Under the new policy, the funding is scheduled to last until May of 2027, before a renewal decision is made.
Some political observers have speculated that the decision to end direct federal funding to community-based organizations could be motivated by the Trump administration’s hostility to diversity, equity, and inclusion or DEI programs and organizations that promote those programs, with the belief that some of the groups receiving the federal HIV prevention funds are promoting DEI.
Carl Schmid, executive director of the D.C.-based HIV+ Hepatitis Policy Institute, is among the leaders of many AIDS advocacy organizations expressing strong opposition to the OMB action. Schmid said that in places like D.C. and some states, local officials will be willing to redirect the federal funds to local community-based organizations.
A list of the 96 community-based organizations across the country that are currently receiving the federal AIDS funds includes the D.C.-based Whitman-Walker Health, which has a long history of healthcare support for the LGBTQ community, and La Clinica del Pueblo, which reaches out to the Latino community.
Schmid said Whitman-Walker and La Clinica del Pueblo have longstanding good relationships with the local D.C. government.
“But other states and jurisdictions don’t have that relationship with the community-based organizations,” Schmid said. “It depends on the state,” he said, adding, “Not all states send their money to the communities that really need it most. And not all states are fast in getting money to the community-based organizations.”
Spokespersons for Whitman-Walker and La Clinica del Pueblo couldn’t immediately be reached for comment on whether they think the Trump administration’s latest action related to funding will adversely impact their respective organizations.
Schmid said under the current federal grant program slated to be discontinued, which has been in effect for at least five years, HIV-related health organizations receiving the federal grant funds were eligible for an existing federal policy enabling them to purchase HIV-related medication, including the PrEP prevention medication, at a significant discount from pharmaceutical companies. With the ending of the direct federal HIV funds to community-based organizations, Schmid said it was unclear whether problems may surface in obtaining drug discounts.
“They could still qualify as a sub-grantee from a state,” Schmid said. “But what if they don’t get that grant again? They would not be able to qualify to obtain the drugs” at the discounted price, he said.
Among the organizations expressing strong concern over the decision to discontinue the direct HIV prevention funding to community-based organizations has been the Federal AIDS Policy Institute and its subgroup called the HIV Prevention Action Coalition.
In a July 22 letter bearing the names of 71 community-based organizations from throughout the country sent to U.S. Department of Health and Human Services Secretary Robert F. Kennedy Jr. and Centers for Disease Control and Prevention Acting Director Jay Bhattacharya, the group called for the Trump administration to “reconsider” ending the current funding policy.
“Ending this program without a clear plan for what comes next would dismantle prevention infrastructure that has taken more than three decades of federal investment to build and do so just as that long record of measurable returns is accelerating,” the letter states.
It says the initiative by President Trump in his first term as president to end the HIV epidemic and reduce new HIV infections by 90 percent by 2030 was moving ahead by the funding program for community-based organizations that the administration now wants to end.
“Discontinuing this program would also cost far more than it saves,” the letter says. “Every HIV transmission prevented avoids an estimated lifetime treatment cost of roughly half a million dollars per person to the healthcare system – costs that fall heavily on taxpayer-funded programs, including Medicaid, Medicare, and the Ryan White HIV/AIDS program,” the letter continues.
“The choice before the administration is straightforward: a modest, targeted investment in prevention now, or far greater public expense for treatment later,” the letter concludes.
Spokespersons for the OMB and the Department of Health and Human Services, which oversees the CDC, have not immediately responded to news media requests for comment on the opposition to the funding change policy.

D.C.’s Mary’s House For Older Adults names new executive director

Suzanne Goode is not good for Rehoboth Beach

Continue to engage in community after Pride month

Doug Ollivant to face Eugene Vindman in Va. 7th Congressional District

LGBTQ advocates optimistic about D.C.’s expected new mayor

Amsterdam Pride Canal Parade draws hundreds of thousands

PHOTOS: Amsterdam Pride Canal Parade

Reggie White relishing first season as artistic director of Woolly Mammoth

Madonna headlines World Pride Music Festival in Amsterdam

PHOTOS: Petal Release Party
-

 Netherlands5 days ago
Netherlands5 days agoAmsterdam Pride Canal Parade draws hundreds of thousands
-
Photos5 days ago
PHOTOS: Amsterdam Pride Canal Parade
-
Theater4 days ago
Reggie White relishing first season as artistic director of Woolly Mammoth
-
Celebrity News4 days ago
Madonna headlines World Pride Music Festival in Amsterdam



