National
Tennessee sends anti-LGBTQ adoption bill to governor’s desk
Governor has already signaled he’d sign religious freedom bill

Adoption legislation in Tennessee opponents say would enable discrimination against LGBTQ families is on its way to the desk of Gov. Bill Lee, who’s expected to the sign the bill in the aftermath of approval Tuesday by the state Senate.
In its first bill of the year, the Tennessee Senate approved HB 836, which would allow adoption agencies to refuse placement into LGBTQ homes on the basis of religious objections. The Senate passed the bill 20-6.
Lee’s office didn’t immediately respond to the Washington Blade’s request to comment on the bill. According to the Tennessean, a Lee spokesperson “confirmed that the governor would be signing the bill as soon as it reaches his desk.”
The bill, sponsored by Sen. Paul Rose (R-Covington), prohibits requiring private licensing child-placement agencies to participate in child placement “that would violate the agency’s written religious or moral convictions.”
The Tennessee House approved the legislation in April 2019, so the measure now heads to the governor’s desk. Despite the report indicating Lee will sign the legislation, LGBTQ advocacy groups are already calling for a veto.
“Passing a bill that funds discrimination in adoption and foster care is one of the worst ways to start a legislative session,” Chris Sanders, executive director of the Tennessee Equality Project, said in a statement. “Despite a vigorous debate on the bill, the best interests of children in Tennessee lost today. We join friends and allies across the country in calling for the governor to veto the bill.”
Although nothing in Tennessee state law or federal law as of now is stopping adoption agencies from refusing placement into LGBTQ homes, the measure could compromise municipal ordinances against anti-LGBT discrimination. According to the 2019 Human Rights Campaign Municipal Index, Tennessee with bans on anti-LGBTQ discrimination in municipal services are Chattanooga, Clarksville, Knoxville, Memphis and Nashville.
The legislation is similar to other laws enacted by other the states in recent years allowing taxpayer-funded adoption agencies to decline to place children into LGBTQ homes over religious objections. Other states are Virginia, Oklahoma, Kansas, Texas, Alabama, Michigan, Mississippi, North Dakota and South Dakota.
Alphonso David, president of the Human Rights Campaign, condemned the Tennessee legislation in a statement for approving the anti-LGBTQ bill.
“Lawmakers in Tennessee used some of the first minutes of their legislative session to enshrine discrimination into law,” David said. “These legislators are disregarding the best interests of kids in the child welfare system to create a ‘license to discriminate’ against qualified, loving prospective parents. This bill does nothing to improve the outcomes for children in care, shrinks the pool of prospective parents and is a blatant attempt to discriminate against LGBTQ Tennesseans. It is shameful that one of the first orders of business in Nashville was to target LGBTQ people. We urge Tennesseans to make their voices heard in opposition to this bill as it heads to the governor’s desk.”




National
Barney Frank on trans rights, 2028, and the need to ‘reform the left’
Gay former congressman starts home hospice care while completing new book
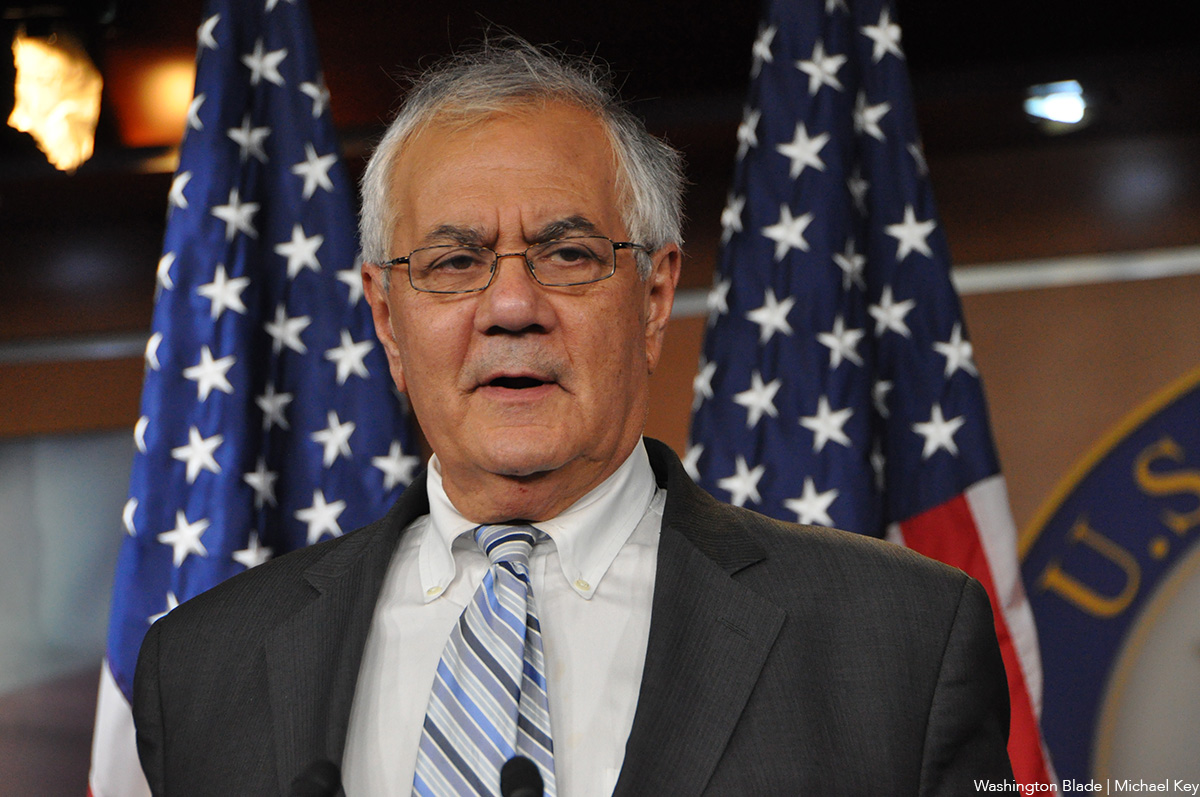
Former U.S. Rep. Barney Frank (D-Mass.), who served in the House from 1981 until his retirement in 2013 and who became the first member of Congress to voluntarily come out as gay in 1987, has resurfaced in the news over the past two weeks after announcing he has entered home hospice care and plans to publish a new book on, among other things, how Democrats can and should regain control of Congress.
According to media reports and an interview Frank conducted this week with the Washington Blade, his book, entitled “The Hard Path to Unity: Why We Must Reform the Left to Rescue Democracy,” calls on the Democratic Party’s progressive left leaning members to be more strategic in pushing for laws and policies initially considered “politically unacceptable” to most U.S. voters and the American people.
Frank told the Blade he believes the LGBTQ rights movement has succeeded in advancing most of its agenda seeking protections against discrimination by initially pushing less controversial advances such as the end to the ban on gays in the military and non-discrimination in employment before taking on the more controversial issue of same-sex marriage.
While acknowledging that Congress has yet to pass a national law banning discrimination against LGBTQ people in employment, housing, and public accommodations as 22 states and D.C. have already done, he points to the two landmark U.S. Supreme Court decisions, one legalizing same-sex marriage nationwide in Obergefell v. Hodges in 2015, and the other declaring sexual orientation and gender identity are protected categories for which employment discrimination is prohibited under existing federal law in Bostock v. Clayton County in 2020.
Frank notes that while some in the LGBTQ community are fearful that LGBTQ rights are under attack and may be pulled back under the Trump administration, he believes Republicans in Congress at this time will not attempt to repeal any existing LGBTQ protections, especially those regarding marriage rights and employment protections secured by the Supreme Court rulings.
He says transgender rights are the remaining LGBTQ issue that have yet to be adopted rationally, and he fully supports ongoing efforts to advance trans rights. But like his criticism of the progressive left among Democrats, Frank says the efforts to advance trans rights could be jeopardized by the highly controversial issue of “male to female transgender people playing in women’s sports.”
He added, “That’s the most controversial, the most difficult. It affects the fewest number of people.” While he says trans rights supporters should continue to advocate for that, “they should not make it a litmus test and say well if you’re not for that you’re not a supporter of the rights of transgender people. There are places where people are supportive, and we want to encourage that.”

Frank, 86, told Politico he has entered home hospice care as he deals with ongoing congestive heart failure. He said he is remaining in his home in Ogunquit, Maine, where he has lived with his husband, Jim Ready, since retiring from Congress in 2013.
“I’ve been doing some writing. I wrote this book,” Frank told the Blade. “I’ve relaxed. Meanwhile, my health has been failing. Jim has been a saint in taking care of me,” he said. “And so, I take it easy.”
Frank spoke to the Washington Blade in a phone interview from his home on May 4.
Washington Blade: We’re hearing some interesting reports about the book you’ve been writing. Can you say when it will be published?
Barney Frank: Sept. 15 is the publication date.
Blade: Some of the reports about the book in the media have said you want the far left within the Democratic Party to be more cautious.

Frank: No, I’ll give you this. The job is to defeat populism to keep democracy. Clearly you have to know what caused it. I believe that the essential cause in the surge of populism was economic inequality and the failure of mainstream liberals to address inequality. And beginning in the ‘80s economic growth became less and less fair in its institutions. And that led to all this anger.
So, the mainstream left finally figured that out after [Bernie] Sanders and Trump in ’16. So, we then – because I was working to make that change – got the Democrats to pay attention to economic inequality. And Joe Biden’s program did. The problem is at that point, people on the left who had correctly been critical of the failure to address equality said, OK, that’s not the only problem you guys are missing. There are all these other problems.
And they jumped from being right on the question of inequality and equality to believing in a lot more social changes, some of which were just unacceptable to the public. And the mistake they make is they don’t distinguish – there are a lot of issues I’ve been for in my life, but I had to assert that they were not currently politically survivable.
So, you do two things. Those that are politically survivable work to get them done. Others, you become an advocate. But you don’t make the most controversial part of your agenda litmus tests and drive away your allies. You will remember that on marriage that was an issue and in 2000 they insisted you will be for marriage.
So, my thesis is that while the mainstream understood its mistake on inequality, the most militant and ideological of our left misunderstand public opinion and they are pushing the public to — and they are insisting on acceptance of things that are not politically acceptable.
Blade: Having said what you said, how do you see that impacting gay rights or LGBTQ rights?
Frank: Well in the first place, gay rights – one of the things I want to address – is this fear that gay rights are going to be taken away – rights for LGB people. Nonsense. We’re not going to lose any of those rights. If they tried to undo marriage, for instance, the political reaction they would get would be abortion type sentiment. They are just not going to do that because it causes them too many political problems.
The problem is advances we hope to make in the area of transgender people. But there is no chance of losing – I can’t think of a single right that is in jeopardy. They are not going to reintroduce the ban in the military. They’re not going to tell people their marriages are cancelled. Again, the Republicans are not even trying to do that because they know there would be a terrible backlash.
With regard to LGBT there is one analogy. And that is the most controversial issue we faced over the years on what was the gay-bisexual agenda was same-sex marriage. And we left that until the end. And you remember we did the military. We did ENDA. We moved on to everything else, and it wasn’t until the very end that we went into marriage. [NOTE: ENDA did not ultimately pass.]
I think the analogy to that is male to female transgender people playing in women’s sports. That’s the most controversial, the most difficult. It affects the fewest number of people. And I believe had we deferred on marriage — people who believe that’s important should advocate for it. But they should not make it a litmus test and say well if you’re not for that you’re not a supporter of the rights of transgender people. There are places where people are supportive, and we want to encourage that.
Blade: You said you don’t think we will lose any rights, most of the laws related to nondiscrimination are from the states or municipal laws that were passed.
Frank: Tell me what you think will be lost. You and I always have this problem. I’ve always felt you were cynical and skeptical. Tell me what right we now have that’s in jeopardy.
Blade: One would be if the Supreme Court reverses its decision on same-sex marriage.
Frank: If they do, Congress would now step in on that, which would be the passage of Tammy Baldwin’s bill.
Blade: But what I was going to ask you next is in all the years you’ve been in office and as of now a federal LGBTQ rights bill has not been passed by Congress yet. Is there a chance of that happening?
Frank: I do not think it will happen because the members of Congress do not want to be in the position of voting to cancel people’s marriages. There are valid marriages throughout the country. And the notion that Congress will pass a bill invalidating those, no they won’t. They won’t do anything that’s as disruptive and that will cause a strong reaction. Have you seen a federal bill to do that? I haven’t.
Blade: No, and I am sorry if I’m not putting the question across correctly. I’m talking about the bill that bans discrimination based on employment, public accommodations and other areas for LGBTQ people that Congress has not yet passed. You co-sponsored that for many years.
Frank: I know that, and the Supreme Court did that one. No, I don’t think that – oh, all right, that’s a different question than marriage. If the Supreme Court reverses itself on that – I don’t see any sign that they’re going to, then I think you would see the federal bill passed.
[He is referring to the 2020 U.S. Supreme Court decision that employment discrimination against gay, bi, and trans people was equivalent to sex discrimination, which is prohibited under Title VII of the Civil Rights Act of 1964.]
Blade: Are you talking about marriage?
Frank: For both for marriage and for non-[discrimination] – I don’t think a marriage bill would pass nationally. To distinguish, I don’t think a bill striking down marriages would pass. Too much violent reaction. As to employment discrimination, where they haven’t acted yet, if the Supreme Court changes that – I think that’s extremely unlikely – then I think Congress would step in.
Blade: Are you saying we may not need an LGBTQ non-discrimination act by Congress for the states that haven’t passed that?
Frank: I would be in favor of that, yes. But again, I think you and I – you have always been pessimistic. There is a political time now that works in our favor. And as I said, on abortion, they burned themselves very badly on abortion. And yes, I’m still for a national anti-discrimination bill. But I do not think the right wing wants to be caught taking rights away that already exist. Because that’s a lot harder than denying them in the first place. And I don’t see any movement for that. You tell me what you are worried about. What bills are you worried about?
Blade: I was simply saying they haven’t yet passed a federal non-discrimination bill.
Frank: No, what’s going to change on the Supreme Court? I don’t see a pretty quick reversal on the Supreme Court. So, I think people are just – they have to have a cause. And they are inflating the likelihood that we are going to lose some rights when I see no evidence of it. And in fact, I see a lot of political reasons why those in Congress don’t want to do that.
I’ll tell you there are a lot of Republicans who would vote for same-sex marriage. For example, the leadership would say for Christ’s sake, don’t bring that up. They don’t want to take a position on it. And they got burned on abortion, badly.
Blade: To the extent that you are observing this, do you think the LGBTQ rights organizations are doing what they should be doing?
Frank: Well, I think some are stressing the negative too much. Because when people believe nothing good ever happens, they may get discouraged. I think they should be concentrating on the transgender issue. And I know the most controversial parts are protecting people’s rights to medical care, their rights selecting their own gender. And that’s what I would be working on.
And yeah, it would be nice to pass the national bill. I don’t think that’s going to happen. Well, if the Democrats get the House, the Senate, and the presidency, maybe it will happen. But I don’t see the urgency of that because I don’t see any movement to reverse the Supreme Court’s decision.
Blade: What message would you have for the LGBTQ community?
Frank: My message is one, we’re in good shape. And two, that what remains in the transgender issue – who is first? Which are those of your issues that are the most politically acceptable. And you work your way through and as you win on some of those the resistance on the tougher ones will diminish. And the other issue is we are – the problem is the stand to protect the rights of transgender people. But the rights for lesbian, gay, and bisexual people, I do not think they are in jeopardy and I do not think a lot of resources should be spent on being what I think is a very small threat.
Blade: For those states and municipalities that do not have laws protecting LGBTQ people from discrimination, do you think attitudes are changing so there would be little or no discrimination?
Frank: Oh, no question. First of all, I think it’s very unlikely that any of the rights they have will be taken away. And secondly, if they had to take some positive steps to take away protections they would not do it. And I think that ship has sailed in our direction and isn’t going back. In the end, you cannot underestimate there’s a big political difference between denying people their rights in the first place and taking it away from them after they’ve enjoyed it.
Anything is theoretically possible, but I don’t see any evidence that’s likely to happen.
Blade: We’re coming up to the midterm elections this year, but is there anyone coming up in the next presidential election who you might be supporting?
Frank: Oh, I think at this point we’re going to have a fairly open Democratic process. And it’s very clear at this point the way American politics is going it will be a basically supportive Democrat against a basically opposed Republican. And I’ll be supporting the Democrat. And so, this Democrat would be the best one, the most electable. And which one, I haven’t decided that. I want to see how people will fare when they start running.
But I think it is inconceivable that the Democrats would nominate someone who is not fully supportive.
Blade: Some people might be asking what you have been doing since you retired from Congress.
Frank: I’ve been doing some writing. I wrote this book. I’ve relaxed. Meanwhile, my health has been failing. Jim [husband Jim Ready] has been a saint in taking care of me. And so, I take it easy. In terms of what I do, I have two rules, two pieces of advice for people who retire. One is that you should make up two lists. One is you should have a bucket list, a list of things you want to do before you’re through. But more important than the bucket list is a list that rhymes with bucket. That’s a very important list. And that’s one that I increasingly defer to.
Blade: And what is the one other than bucket?
Frank: It rhymes with bucket. What rhymes with bucket?
Blade: Oh, OK.
Frank: That’s the list I follow.
Florida
Key West Pride’s state funding pulled
Republican Fla. Gov. Ron DeSantis signed anti-DEI bill

Following the passage of anti-DEI legislation in Florida, Key West will no longer receive any state funding for its future Pride events.
In a letter provided to the Key West Business Guild, the LGBTQ visitor and tourism center for the string of islands, a senior assistant county attorney for Monroe County officially said that the organization would no longer receive funding for its ongoing projects as a result of Senate Bill 1134 and House Bill 1001, starting in 2027.
The popular Key West Pride, gay men–leaning Tropical Heat weekend, and Womenfest will no longer receive any state money. This is something that Gay Key West Visitor Center Executive Director Rob Dougherty highlighted will shift how all the largest LGBTQ events in the Keys will be held after this year.
He said that the explanation is solely a result of SB 1134 and HB 1001, which limits the official actions of local governments by “prohibiting counties and municipalities, respectively, from funding or promoting or taking official action as it relates to diversity, equity, and inclusion …”
The legislation is being used to impose restrictions on funding events that exclude — whereas the events’ true purpose is to uplift already marginalized groups.
“Womenfest lost it [funding] because it’s a women’s-only event. Tropical Heat lost it because it’s a men’s-only event … that’s how this is being applied.”
This will not impact anything this year, Dougherty assured the Washington Blade; however, the future is not as certain.
“The law that (Republican Florida) Gov. DeSantis signed does not go into effect until Jan. 1, so for 2026 we’re okay,” Dougherty told the Blade. “But it impacts Key West Pride 2027, it impacts Tropical Heat 2027 and Womenfest — so we have lost all funding for those three events.”
He said that this will amount to a large chunk of the expected funding for the LGBTQ celebrations, which the Key West tourism board says is “internationally known as a gay mecca.”
“We’re due to lose about $200,000. Not all of that is direct, but the way that the Tourist Development Council (TDC) distributes their money, about $75,000 of it is for Key West Pride, and that helps to pay for things like marketing, swag, and other things that promote the event.”
He went on to explain that marketing to many major metropolitan areas with large LGBTQ populations may not see the same Key West advertisements and push as in years past — and that is the point.
“Our digital marketing, our print marketing, our SEO marketing — all of that is paid for through there, and it targets places with direct flights like Washington, D.C., New York, Philly, Atlanta, Dallas. So it’s definitely going to impact that.”
The money that will stop coming is not just to run events and celebrations, he explained. Money that goes back directly into the community is going to be hardest hit.
“An estimated 250,000 LGBTQ+ travelers make it to Key West on an annual basis, and on a very conservative basis, for every LGBTQ+ person there are two to four allies traveling with the same values.”
“The TDC also estimates that $1,500+ is spent per person per visit … so if you take those figures and multiply those all together, it comes up to about $1.2 billion … that is potentially going to be lost.”
He says that this will intrinsically change how Key West’s tourism — especially the large LGBTQ side of it — will run, especially since gay vacations need a foundation and expectation of safety and support to blossom.
“We travel based upon where we feel most welcome,” Dougherty said. “Key West has always been its own little place … the LGBTQ+ history of Key West and everything about Key West has always been a little bit weird for people, and that’s why they come here.”
The Guild was formed in 1978 to encourage summer tourism and support Key West’s gay community — becoming the nation’s first LGBTQ destination marketing organization. It has grown tremendously from its original membership to now include more than 475 enterprises representing virtually every facet of the island’s business community.
He also went on to say that this should be eye-opening for anywhere considered an LGBTQ destination, regardless of whether it is in a blue state or a red one.
“I think it can be a wake-up call across the country, because if it can happen here, it can happen anywhere.”
Federal Government
DOE investigates Smith College’s trans-inclusive policy
Mass. college accused of violating Title IX

The U.S. Department of Education announced on Monday that it opened an investigation into Smith College for admitting transgender women.
Smith College, a private and famously all-women’s college in Northampton, Mass., established in 1871 and opened in 1875, has a long list of women who make up its historic alumni — including first ladies, influential political figures, and cultural leaders.
The DOE released a statement about the investigation into the institution through the Department’s Office for Civil Rights, saying it was looking into the possibility that Title IX of the Education Amendments of 1972 was violated by allowing trans women, referred to in the statement as “biological males,” into women’s intimate spaces protected by IX.
The statement explicitly highlighted that this stems from trans women being granted “access to women-only spaces, including dormitories, bathrooms, locker rooms, and athletic teams” while also allowing their audience into the school itself.
This is the first time the Trump-Vance administration has taken a step into admissions processes, a stark jump past investigating policies that allowed trans women to participate in women’s sports and use women’s bathrooms, and allows for the administration to go more after trans acceptance policy as a whole.
Smith’s admission policy allows for “any applicants who self-identify as women,” including “cis, trans, and nonbinary women,” according to the college’s website, and has since 2015, when it updated its policy.
“The college is fully committed to its institutional values, including compliance with civil rights laws,” Smith’s statement in response to the DOE’s investigation said. “The college does not comment on pending government investigations.”
“An all-women’s college loses all meaning if it is admitting biological males,” said Assistant Secretary for Civil Rights Kimberly Richey. “Allowing biological males into spaces designed for women raises serious concerns about privacy, fairness, and compliance under federal law. The Trump administration will continue to uphold the law and fight to restore common sense.”
This move continues to align with actions the Trump-Vance administration has taken to curtail LGBTQ — and specifically trans — rights in America, as members of the administration attempt to break down safeguards and protections that have long been used to protect marginalized communities.
Since Trump took office in his second term, there have been significant legal challenges. According to the National LGBTQ+ Bar Association, there are over 35 court cases that have emerged since his second swearing-in that directly relate to the administration’s attempts to minimize the rights and protections of trans Americans — from medical care and educational protections to military policy.
Much of this anti-trans policy direction was outlined beginning in 2022 with the Project 2025 playbook, which Trump officials have used as a guide to scale back protections for LGBTQ people, Black Americans, poor and Indigenous communities, while also increasing costs for lower-income Americans and providing tax cuts to the wealthy and ultra-wealthy. The plans also “erode” Americans’ freedoms and remove crucial checks and balances that have allowed the executive branch to remain in line with the Constitution without becoming too powerful over either the courts or the legislative branch.

New Hungarian prime minister takes office

Comings & Goings

Learn more about queer love

Calendar: May 8-14

Va. Supreme Court invalidates Democrat-backed redistricting plan

How do you vote a child out of their future?

Gay ICE detainee freed after 150 days in detention

A reign defined by commitment and human impact

Ukrainian MPs advance new Civil Code without protections for same-sex couples

DOE investigates Smith College’s trans-inclusive policy
-

 Commentary5 days ago
Commentary5 days agoHow do you vote a child out of their future?
-
New York5 days ago
Gay ICE detainee freed after 150 days in detention
-
Arts & Entertainment4 days ago
A reign defined by commitment and human impact
-
Ukraine4 days ago
Ukrainian MPs advance new Civil Code without protections for same-sex couples



