National
HIV research sped development of COVID vaccine
Top NIH official says success in coronavirus will boost AIDS work

Since 1996, Carl W. Dieffenbach, who holds a Ph.D. in biophysics from John Hopkins University, has served as director of the Division of AIDS at the National Institute of Allergies and Infectious Diseases, which is an arm of the U.S. National Institutes of Health or NIH.
In a June 10 interview with the Washington Blade, Dieffenbach gave an update on the extensive, ongoing research into the development of an HIV/AIDS vaccine that he has helped to coordinate for many years, including current human trials for a prospective AIDS vaccine taking place in the U.S., South America, and Africa.
One thing he feels passionate about is a development not widely reported in the media reports about the successful development of the COVID-19 vaccine. According to Dieffenbach, the extensive research into an AIDS vaccine in recent and past years, while not yet successful in yielding an effective AIDS vaccine, helped lay the groundwork for the rapid development of the different versions of a COVID vaccine.
“Because my division runs the largest clinical trials program in the word, we jumped in with both feet to help with coronavirus disease for both vaccines and drugs and things like that,” he said. “And the platforms that were used – the way they are making the coronavirus vaccines – the RNA vaccines with Moderna – were first piloted by NIH and Moderna to try to make an HIV vaccine,” Dieffenbach says.
“So, in many ways, the work for the past 25 years that we’ve done in HIV vaccines sped the development of coronavirus vaccines,” he told the Blade. “And now it’s time to take what we’ve learned from coronavirus and take it back to HIV and start afresh or continue with what we have and build upon from what we have learned.”
Dieffenbach says one reason the development of a COVID vaccine came about before an AIDS vaccine, despite more than 20 years of AIDS vaccine research, is that the HIV virus is far more complex than the coronavirus, especially its ability to infect and remain embedded in the infected person for life.
“Back in 2007 we had the first hint that an AIDS vaccine might be possible with a study called RV144,” Dieffenbach says. “We spent 10 years trying to replicate that, and we just completed that study – a study called HVTN702. And it showed no efficacy,” he said, meaning it did not work.
“So that was a big disappointment to us,” he says “But in the meantime, we had pushed forward with the J&J [Johnson and Johnson pharmaceutical company] vaccine and are pretty far along. We’ll see what happens. We should know in the next several months whether the N26 version of an AIDS vaccine, and HIV vaccine works or not,” he says. “We’re very close to an answer.”
Washington Blade: Where do things stand in the development of an HIV/AIDS vaccine in light of Dr. Fauci’s statement a few weeks ago that the development of a COVID-19 vaccine could provide a boost to developing an AIDS vaccine?
Carl Dieffenbach: Sure. So, maybe I can start by introducing myself to you as a way of putting this into a context.
So, I’m the director of the Division of AIDS, which is the largest funder of HIV research in the world. And I report directly to Dr. Fauci. So, I’m responsible for all AIDS, all the time. And that is my passion and purpose in life. Part of that is working toward a safe, effective, and durable HIV vaccine, which has been one of the two most challenging questions left in science today. The other is a cure. They are connected in some ways.
So, with that as background, when coronavirus disease came along – because my division runs the largest clinical trials program in the world – we jumped in with both feet to help with coronavirus disease for both vaccines and drugs and things like that. And the platforms that were used – the way they are making the coronavirus vaccines – the RNA vaccines with Moderna were first piloted by NIH and Moderna to try to make an HIV vaccine. So, we’ve being working on that platform with Moderna for several years.
The leadership at Pfizer used to be part of a group at Penn, where we were also working with them. The J&J vaccine – we currently have in two Phase III clinical trials for HIV, one in sub-Saharan Africa, specifically in young women and the other one in the Americas in men who have sex with men and transgender individuals. Both of those Phase IIIs are moving along. The women’s study is fully enrolled. The men’s study was hit hard by COVID, but we worked through and will be fully enrolled by September.
One other vaccine just to talk about is the Oxford vaccine, the AstraZeneca vaccine. That is also using a platform at Oxford University, which has been used for HIV. So, in many ways, the work for the past 25 years that we’ve done in HIV vaccines sped the development of coronavirus vaccines. And now it’s time to take what we’ve learned from coronavirus and take it back to HIV and start afresh or continue with what we have and build upon from where we have learned.
Blade: That’s very interesting. But can we assume, then, from the clinical trials that have taken place for an HIV vaccine that they did not succeed in providing the immunity needed for an effective vaccine?
Dieffenbach: So, that’s exactly the problem we have. Back in 2007 we had the first hint that an AIDS vaccine might be possible with a study called RV144. We spent 10 years trying to replicate that, and we just completed that study – a study called HVTN702. And it showed no efficacy. So, that was a big disappointment to us. But in the meantime, we had pushed forward with the J&J vaccine and are pretty far along. We’ll see what happens. We should know in the next several months whether the N26 version of an AIDS vaccine, and HIV vaccine works or not. We’re very close to an answer.
Blade: So, the human trials are ongoing.
Dieffenbach: Oh, again – the study in young women in sub-Sahara Africa is fully enrolled. The men’s study will be fully enrolled in September. So, we have fought through the coronavirus epidemic to maintain, to nurse these trials along to make sure with the $100 million or so we’ve invested, that we didn’t want them to go down the drain literally because we lost too many people for follow-up. So, this was a herculean effort that has gone on all the time trying to do the vaccine studies for coronavirus disease, which we were also incredibly successful in.
Blade: Can we assume all of the people participating in the studies were HIV negative?
Dieffenbach: Yes, they’re HIV negative. They are people who are at risk. And also, in South America, for example, the major countries we’re in are Peru and Brazil. And they’ve had a strong research culture with us, going back more than a decade. For example, both of those countries played big roles in our studies of pre-exposure prophylaxis. A study called I-PREX that demonstrated that in men who have sex with men that [a PrEP drug] works well to prevent HIV acquisition in seronegative men who have sex with men.
So, we’ve been there. This is a really good setup for the countries, for the citizens that are in those countries that want to avail themselves to the research that has benefited everybody.
Blade: Among those who are participating in these ongoing AIDS vaccine trials, can we assume they cannot be taking the PrEP anti-retroviral drugs that have been shown to be highly effective in preventing HIV infection?
Dieffenbach: So, what we’ve done is we – everything is by conversation. So, when somebody who is interested in the study comes in, we talk to them. What is your chief interest in being in this study? And a lot of people want to be in the study because then they can access PrEP. They want to make it easier to get a hold of pre-exposure prophylaxis. They feel that is the best way that they can protect themselves.
So, in that situation, what we do is we take those people and link them to PrEP services where they can easily get PrEP in their community. So, first it’s taking care of those people. Then there are people who really have no interest in PrEP. And we actually counsel them every time they come in for a study. Are you sure you don’t want to access PrEP? And those are the people we then say, if you’re not interested in PrEP, what do you think about participating in a vaccine trial?
Because they’re the ones who have the most freedom of thought. They don’t have an opinion about the vaccine or about PrEP. So, those are the people we’ve been focusing on and enrolling. So, we’ve been very careful to make sure that if people wanted PrEP they not only have access, but they didn’t feel like somehow having to trade something in order to get it. The freedom to join a study should be a free choice. And it shouldn’t be a coercive thing to get PrEP. So, we just took that off the table and said if you’re truly interested in PrEP we can get you PrEP and make sure that was available.
Blade: So, in that case, if they choose PrEP they would not be in the vaccine trial?
Dieffenbach: You know, it’s interesting that you ask it in that way. Because you have relationships with your community, many of the investigators have reported that people will say, you know I tried PrEP and it wasn’t for me. It made me gaseous. It upset my stomach. I wasn’t myself. I tried it. I couldn’t make it work for me. I want to stop PrEP. Am I still eligible for the [vaccine] study? And the answer is of course. Many people are very happy on PrEP and they come in for visits occasionally and say this is working for me and just have the relationship with the doctors there, so it works. So, again, it’s about maintaining contact with your communities.
Blade: Can you tell a little about what happens next after people become part of an HIV vaccine trial. Do you have to keep in touch with these people, and do they have to get an HIV test periodically?
Dieffenbach: Exactly. So, the vaccine consists of a series of injections. It’s a mixture of vector systems that delivers a series of encoded HIV genes that are specifically designed to induce very broad immunity. There’s a whole computer-based process to design those components of the vaccine to make sure that it has sequence similarities with all the different versions of HIV circulating in the globe. And then at the end there is a protein boost. And we carry this out.
So, about every three to four months people come in. They get a shot. They fill out questionnaires. They give a blood sample. And they’re tested for HIV and are given a boost or a placebo. And they stay in touch with the clinic. They come in and out of the clinic. And the retention is quite high in these situations because people really like having the attention of the clinic available to them. It’s part of the community.
Blade: So, they go to a clinic for all of this?
Dieffenbach: It’s a research clinic. It’s not like a state-run health clinic. It’s a research clinic. Clinic is just a term for where people are seen.
Blade: Are any of these AIDS vaccine trials that are going on taking place in the United States?
Dieffenbach: Yes. So, the study is called Mosaico. And it’s HVTN706. And we have sites throughout the United States as well as South America. But that study is limited to men who have sex with men – the one in the United States.
Blade: Is it broader than just men who have sex with men in other countries?
Dieffenbach: No, so we decided to really focus on specific at-risk populations. So, in the Americas we chose to focus on men who have sex with men and transgender individuals. And sub-Saharan Africa we focused on young women because that is the target of the study population. So, 705 is all women in sub-Saharan Africa. And in the Americas in North and South America it is all men who have sex with men and transgender individuals.
Blade: Can we assume that the researchers that are doing these studies have a sensitivity of LGBTQ people? Is there still an issue where people worry about being outed as being gay or transgender?
Dieffenbach: So, many of the sites that we work with have been part of our system for over 20 years. And so, they are trusted members of the LGBTQ community within their cities and states. And ‘states’ is a literal term where it’s a state in Colombia or Peru or Brazil. And so, it is part of the fabric of the gay community in these places. Just like in San Francisco the San Francisco health clinic and the DCF clinics are part and parcel of everything the community does there.
And so, the lead physician in San Francisco is Susan Buchbinder. She has been a leader in health in this population for over 25 years or actually closer to 30 years at this point. We’re all getting old. Do you know that? So, we have been at this a very long time. And really have tried to build structures that are durable and therefore are reliable to the community. And that’s where we go back to the same groups time after time.
Blade: Have the locations of the vaccine testing sites been released publicly?
Dieffenbach: Yes, all of that is publicly available on clinicaltrials.gov. If you go into clinicaltrials.gov and search HVTN705 or HVTN706 you will get a version of the protocol, all the times it’s been modified, where we are – the protocol. All of that is public knowledge and available to you. HVTN705 is the women’s study. HVTN706 is the men’s study.
Blade: Is there a timeframe for when these latest vaccine studies might be completed?
Dieffenbach: I think within the next several months. We will get an answer out of the women’s study and then the men’s study is probably a year away. We were slowed a little bit because of COVID. We actually had to pause enrollment for several months. But we’re back on track.
Blade: Isn’t there a parallel research effort for an HIV/AIDS cure?
Dieffenbach: Yes, we have a very large program in cure research. It is a lot earlier in the discovery process and so it’s still very ‘researchy.’ And we have a very large program called the Martin Delany Collaboratories for Cure Research. Martin Delany was an activist who really pushed NIH in so many wonderful ways to really take the need for a cure seriously. His argument was a cure is the next logical step after effective anti-retroviral therapy. You cannot stop with one pill once a day. You’ve got to keep going. And he was pretty persistent. And unfortunately, he died several years go and we just thought the best way to honor him, and his memory was to name a program after him.
Editor’s note: Next week, in the second and final installment of his interview with the Blade, Dr. Dieffenbach discusses the progress in research and studies into an HIV/AIDS cure and explains from a scientific standpoint why an HIV vaccine is taking longer to develop than a COVID vaccine.




National
United Methodist Church removes 40-year ban on gay clergy
Delegates also voted for other LGBTQ-inclusive measures

The United Methodist Church on Wednesday removed a ban on gay clergy that was in place for more than 40 years, voting to also allow LGBTQ weddings and end prohibitions on the use of United Methodist funds to “promote acceptance of homosexuality.”
Overturning the policy forbidding the church from ordaining “self-avowed practicing homosexuals” effectively formalized a practice that had caused an estimated quarter of U.S. congregations to leave the church.
The New York Times notes additional votes “affirming L.G.B.T.Q. inclusion in the church are expected before the meeting adjourns on Friday.” Wednesday’s measures were passed overwhelmingly and without debate. Delegates met in Charlotte, N.C.
According to the church’s General Council on Finance and Administration, there were 5,424,175 members in the U.S. in 2022 with an estimated global membership approaching 10 million.
The Times notes that other matters of business last week included a “regionalization” plan, which gave autonomy to different regions such that they can establish their own rules on matters including issues of sexuality — about which international factions are likelier to have more conservative views.
Rev. Kipp Nelson of St. Johns’s on the Lake Methodist Church in Miami shared a statement praising the new developments:
“It is a glorious day in the United Methodist Church. As a worldwide denomination, we have now publicly proclaimed the boundless love of God and finally slung open the doors of our church so that all people, no matter their identities or orientations, may pursue the calling of their hearts.
“Truly, all are loved and belong here among us. I am honored to serve as a pastor in the United Methodist Church for such a time as this, for our future is bright and filled with hope. Praise be, praise be.”
Federal Government
Republican state AGs challenge Biden administration’s revised Title IX policies
New rules protect LGBTQ students from discrimination

Four Republicans state attorneys general have sued the Biden-Harris administration over the U.S. Department of Education’s new Title IX policies that were finalized April 19 and carry anti-discrimination protections for LGBTQ students in public schools.
The lawsuit filed on Tuesday, which is led by the attorneys general of Kentucky and Tennessee, follows a pair of legal challenges from nine Republican states on Monday — all contesting the administration’s interpretation that sex-based discrimination under the statute also covers that which is based on the victim’s sexual orientation or gender identity.
The administration also rolled back Trump-era rules governing how schools must respond to allegations of sexual harassment and sexual assault, which were widely perceived as biased in favor of the interests of those who are accused.
“The U.S. Department of Education has no authority to let boys into girls’ locker rooms,” Tennessee Attorney General Jonathan Skrmetti said in a statement. “In the decades since its adoption, Title IX has been universally understood to protect the privacy and safety of women in private spaces like locker rooms and bathrooms.”
“Florida is suing the Biden administration over its unlawful Title IX changes,” Florida Gov. Ron DeSantis wrote on social media. “Biden is abusing his constitutional authority to push an ideological agenda that harms women and girls and conflicts with the truth.”
After announcing the finalization of the department’s new rules, Education Secretary Miguel Cardona told reporters, “These regulations make it crystal clear that everyone can access schools that are safe, welcoming and that respect their rights.”
The new rule does not provide guidance on whether schools must allow transgender students to play on sports teams corresponding with their gender identity to comply with Title IX, a question that is addressed in a separate rule proposed by the agency in April.
LGBTQ and civil rights advocacy groups praised the changes. Lambda Legal issued a statement arguing the new rule “protects LGBTQ+ students from discrimination and other abuse,” adding that it “appropriately underscores that Title IX’s civil rights protections clearly cover LGBTQ+ students, as well as survivors and pregnant and parenting students across race and gender identity.”
Federal Government
4th Circuit rules gender identity is a protected characteristic
Ruling a response to N.C., W.Va. legal challenges

BY ERIN REED | The 4th U.S. Circuit Court of Appeals ruled Monday that transgender people are a protected class and that Medicaid bans on trans care are unconstitutional.
Furthermore, the court ruled that discriminating based on a diagnosis of gender dysphoria is discrimination based on gender identity and sex. The ruling is in response to lower court challenges against state laws and policies in North Carolina and West Virginia that prevent trans people on state plans or Medicaid from obtaining coverage for gender-affirming care; those lower courts found such exclusions unconstitutional.
In issuing the final ruling, the 4th Circuit declared that trans exclusions were “obviously discriminatory” and were “in violation of the equal protection clause” of the Constitution, upholding lower court rulings that barred the discriminatory exclusions.
The 4th Circuit ruling focused on two cases in states within its jurisdiction: North Carolina and West Virginia. In North Carolina, trans state employees who rely on the State Health Plan were unable to use it to obtain gender-affirming care for gender dysphoria diagnoses.
In West Virginia, a similar exclusion applied to those on the state’s Medicaid plan for surgeries related to a diagnosis of gender dysphoria. Both exclusions were overturned by lower courts, and both states appealed to the 4th Circuit.
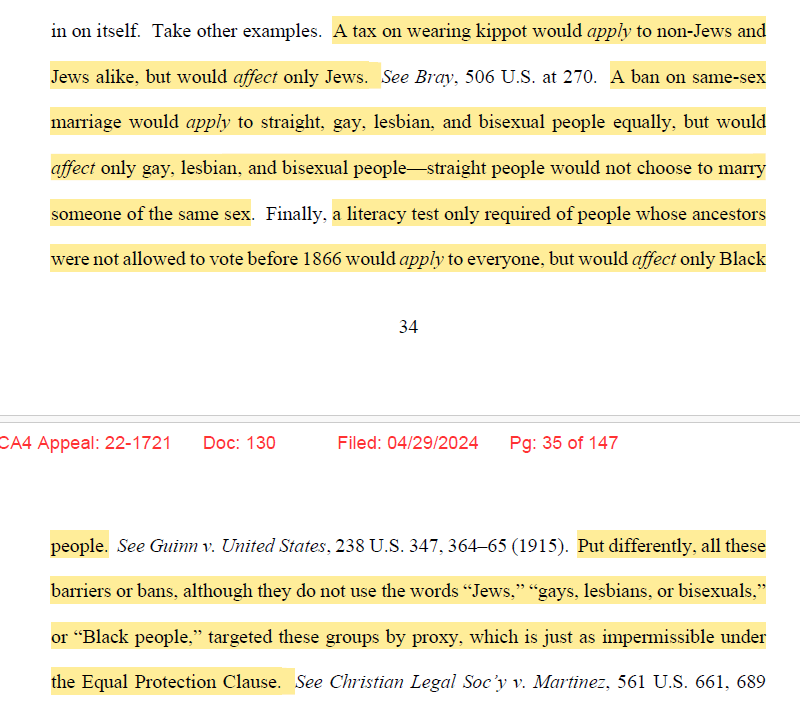
Attorneys for the states had argued that the policies were not discriminatory because the exclusions for gender affirming care “apply to everyone, not just transgender people.” The majority of the court, however, struck down such a claim, pointing to several other cases where such arguments break down, such as same-sex marriage bans “applying to straight, gay, lesbian, and bisexual people equally,” even though straight people would be entirely unaffected by such bans.
Other cases cited included literacy tests, a tax on wearing kippot for Jewish people, and interracial marriage in Loving v. Virginia.
See this portion of the court analysis here:
Of particular note in the majority opinion was a section on Geduldig v. Aiello that seemed laser-targeted toward an eventual U.S. Supreme Court decision on discriminatory policies targeting trans people. Geduldig v. Aiello, a 1974 ruling, determined that pregnancy discrimination is not inherently sex discrimination because it does not “classify on sex,” but rather, on pregnancy status.
Using similar arguments, the states claimed that gender affirming care exclusions did not classify or discriminate based on trans status or sex, but rather, on a diagnosis of gender dysphoria and treatments to alleviate that dysphoria.
The majority was unconvinced, ruling, “gender dysphoria is so intimately related to transgender status as to be virtually indistinguishable from it. The excluded treatments aim at addressing incongruity between sex assigned at birth and gender identity, the very heart of transgender status.” In doing so, the majority cited several cases, many from after Geduldig was decided.
Notably, Geduldig was cited in both the 6th and 11th Circuit decisions upholding gender affirming care bans in a handful of states.
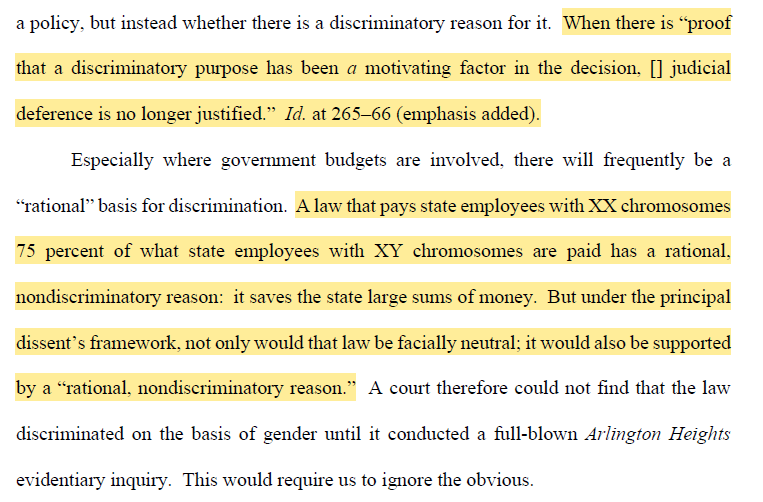
The court also pointed to the potentially ridiculous conclusions that strict readings of what counts as proxy discrimination could lead to, such as if legislators attempted to use “XX chromosomes” and “XY chromosomes” to get around sex discrimination policies:
Importantly, the court also rebutted recent arguments that Bostock applies only to “limited Title VII claims involving employers who fired” LGBTQ employees, and not to Title IX, which the Affordable Care Act’s anti-discrimination mandate references. The majority stated that this is not the case, and that there is “nothing in Bostock to suggest the holding was that narrow.”
Ultimately, the court ruled that the exclusions on trans care violate the Equal Protection Clause of the Constitution. The court also ruled that the West Virginia Medicaid Program violates the Medicaid Act and the anti-discrimination provisions of the Affordable Care Act.
Additionally, the court upheld the dismissal of anti-trans expert testimony for lacking relevant expertise. West Virginia and North Carolina must end trans care exclusions in line with earlier district court decisions.
The decision will likely have nationwide impacts on court cases in other districts. The case had become a major battleground for trans rights, with dozens of states filing amicus briefs in favor or against the protection of the equal process rights of trans people. Twenty-one Republican states filed an amicus brief in favor of denying trans people anti-discrimination protections in healthcare, and 17 Democratic states joined an amicus brief in support of the healthcare rights of trans individuals.
Many Republican states are defending anti-trans laws that discriminate against trans people by banning or limiting gender-affirming care. These laws could come under threat if the legal rationale used in this decision is adopted by other circuits. In the 4th Circuit’s jurisdiction, West Virginia and North Carolina already have gender-affirming care bans for trans youth in place, and South Carolina may consider a similar bill this week.
The decision could potentially be used as precedent to challenge all of those laws in the near future and to deter South Carolina’s bill from passing into law.
The decision is the latest in a web of legal battles concerning trans people. Earlier this month, the 4th Circuit also reversed a sports ban in West Virginia, ruling that Title IX protects trans student athletes. However, the Supreme Court recently narrowed a victory for trans healthcare from the 9th U.S. Circuit Court of Appeals and allowed Idaho to continue enforcing its ban on gender-affirming care for everyone except the two plaintiffs in the case.
Importantly, that decision was not about the constitutionality of gender-affirming care, but the limits of temporary injunctions in the early stages of a constitutional challenge to discriminatory state laws. It is likely that the Supreme Court will ultimately hear cases on this topic in the near future.
Celebrating the victory, Lambda Legal Counsel and Health Care Strategist Omar Gonzalez-Pagan said in a posted statement, “The court’s decision sends a clear message that gender-affirming care is critical medical care for transgender people and that denying it is harmful and unlawful … We hope this decision makes it clear to policy makers across the country that health care decisions belong to patients, their families, and their doctors, not to politicians.”
****************************************************************************

Erin Reed is a transgender woman (she/her pronouns) and researcher who tracks anti-LGBTQ+ legislation around the world and helps people become better advocates for their queer family, friends, colleagues, and community. Reed also is a social media consultant and public speaker.
******************************************************************************************
The preceding article was first published at Erin In The Morning and is republished with permission.

Brittney Griner considered suicide in Russian prison

Senegalese NGO claims new president discussed LGBTQ rights with top EU official

What Anne Arundel County school board candidates think about book bans

It’s game, set, and mismatch in unfulfilling ‘Challengers’

D.C. Council member proposes change for Mayor’s Office of LGBTQ Affairs

HHS reverses Trump-era anti-LGBTQ rule

4th Circuit rules gender identity is a protected characteristic

PHOTOS: Capital Pride Pageant

New World Bank US executive director: LGBTQ rights are human rights



