Opinions
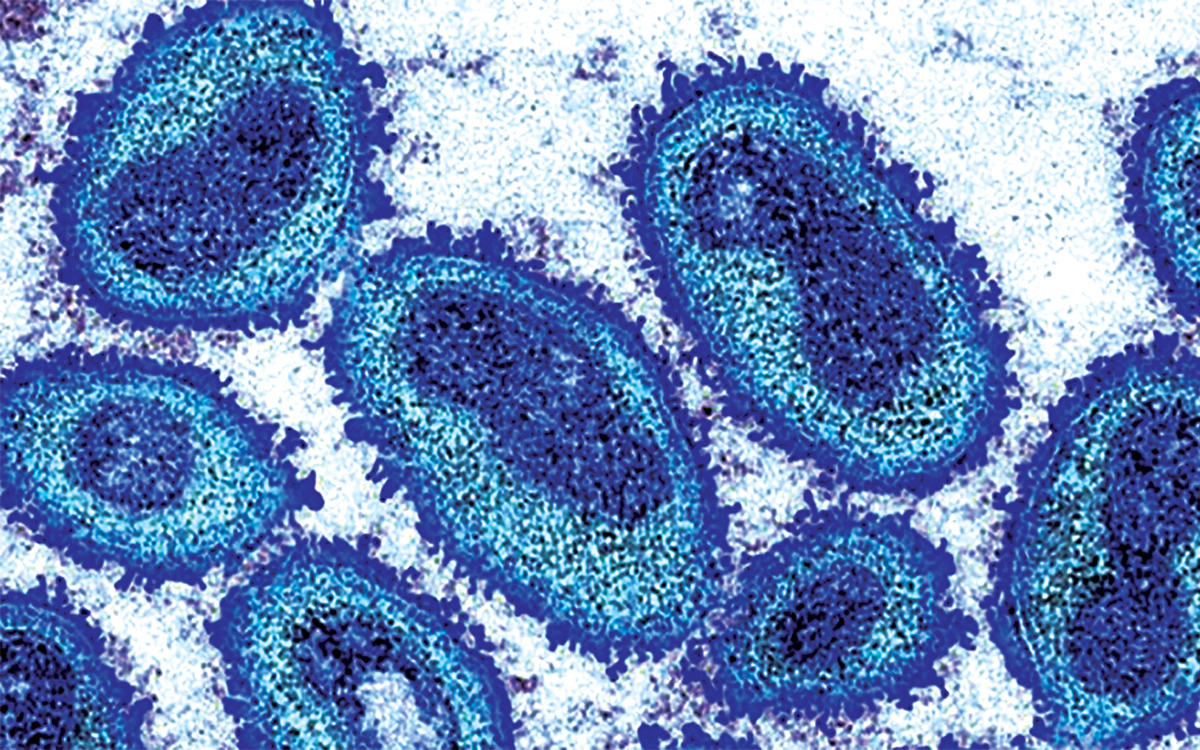
Mpox isn’t gone as virus continues to spread in Africa
A public health issue that transcends identities and borders
By SCOTT BERTANI
Pride is all about celebrating who we are as an LGBTQ+ community. As people. And part of that celebration is making sure we’re taking care of ourselves and looking out for one another. While Pride month may be over, the spirit (and summer) continues.
That’s why this is still an ideal time to talk about health. With so many people still coming together for events and festivities, it’s the perfect opportunity to bring health into the conversation—particularly how essential open communication is when it comes to addressing the current mpox situation.
But communication is a two-way street. Like community, providers need to address health issues like mpox with compassion, competence, and confidence. That means without moralizing, without stigma, and with the trust it takes for people to feel safe and supported when they go back to talk to their partners and friends. The community deserves knowledge and care that reflect our lives.
Mpox, formerly known as monkeypox, is a contagious virus that spreads through close contact, including sex. Though mpox is not a sexually transmitted infection, the patterns are clear: When bodies collide, especially in ways that involve skin-to-skin exposure, transmission can happen. Many people report their first symptoms showing up at sites of sexual contact.
Mpox cases have primarily been seen among sexual and social networks of gay, bisexual, and same-gender-loving men, as well as transgender and nonbinary individuals—especially those with uncontrolled HIV. It has also affected caregivers and women. Because early framing of the virus relied on language and imagery that fueled stigma — particularly toward African nations and then onto LGBTQ+ people — the name change to ‘mpox’ was a deliberate step to correct any unnecessary associations. This is a public health issue that transcends identities and borders, and it deserves a response grounded in science and dignity.
Globally, the concern is growing. In the Democratic Republic of the Congo (DRC), Clade I mpox—historically more severe—has caused more than 48,000 suspected cases and more than 1,100 deaths in 2024, many among children and immunocompromised individuals. A more transmissible subvariant, Clade Ib, has been identified and is now spreading to neighboring countries like Burundi, Kenya, Rwanda, and Uganda, where mpox had not previously circulated. In response, the Africa Centres for Disease Control and Prevention has declared a “public health emergency of continental security.” When diseases like this spread unchecked, the consequences don’t stay confined. What happens globally still affects us locally.
While mpox may not be in the headlines as often as it used to be, it hasn’t gone away. In the United States (U.S.), the Centers for Disease Control (CDC) has confirmed four recent cases of Clade I mpox in individuals with travel history to Africa between late 2024 and early 2025 detected in California, Georgia, New Hampshire, and New York. At this point, there is no evidence of further spread from those cases, and Clade II remains the primary strain circulating in the U.S. However, vaccine uptake is still lagging. Most mpox infections continue to occur among people who are either unvaccinated or only partially vaccinated. For optimal protection, the CDC recommends that those at risk receive two doses of the vaccine to help protect themselves and others from mpox in the midst of a current outbreak. However, just 15 percent of those recommended to get the mpox vaccine have received both doses—leaving significant gaps in protection heading into the summer months.
Vaccination remains one of the most effective tools we have. It not only helps protect against infection, but it can also help reduce symptoms if someone does get sick. The mpox vaccine is highly effective, but it’s a two-part series, and that second dose really matters. Ideally, it’s given at least 28 days after the first—but even if more time has passed, you can always go back at any time.
There are other ways we can all unite this summer during Pride by looking out for ourselves and each other. If you or a partner has a new or unexplained rash or just aren’t feeling right, it’s OK to pause and chat with your doctor. Pay attention to symptoms like painful sores, flu-like symptoms, or discomfort when going to the bathroom. Have open conversations with your partners. If something feels off, don’t wait — reach out to a provider you trust.
So, keep celebrating while staying informed. How we talk and listen to each other, without judgment, is still one of the most powerful ways to protect our health. Happy Pride season all year ‘round!
The National Coalition for LGBTQ Health represents the entire LGBTQ+ community, including clinicians, researchers, service providers, and advocates who serve individuals of every sexual orientation, gender, gender identity, race, ethnicity, and age, regardless of disability, income, education, and geography. The Coalition works to improve LGBTQ health and well-being through advocacy, medical and consumer education, communications, capacity building, and health services research. Learn more at healthlgbtq.org. It also hosts a national Mpox Resource Center (healthlgbtq.org/mpox) and leads “The Q National LGBTQ Health Training Center(healthlgbtq.org/theq), which provides cultural competency training and clinical resources to help providers deliver patient-affirming care. Learn more at healthlgbtq.org.
Scott Bertani is director of advocacy, The National Coalition for LGBTQ Health.





Opinions
Capital Pride must be transparent about sexual misconduct investigation
More questions than answers after two board members resign

We are living through some very difficult times in our country. We have a felon in the White House who has surrounded himself with incompetent sycophants and fascists. A Congress that bows down to him, often based on his threats. Things have gotten so bad that his supporters are beginning to wake up to the fact that he cares not a whit for them. They are demanding he stop hiding his involvement with the convicted sex trafficker, Jeffrey Epstein, and come clean. So, to distract them from this, he began a war in the Middle East in which members of the American military have already lost their lives. He says more lives will be lost. He hopes this war of distraction will have Americans forget his failed domestic policies and the Epstein scandal.
But at the same time that all of this is happening, I am forced to look around at organizations I support and ask if they are being open and honest in the way we are demanding of the felon in the White House.
Recently, I have received calls about an organization I have the utmost pride in: Capital Pride. The calls are about Capital Pride’s internal investigation of “a claim” made against a former board chair, who resigned and no longer has any role with the organization. There has been no public proof of any wrongdoing. At the time, Capital Pride announced it had retained an “independent firm” to investigate the complaint. Now, more than four months later, a second board member has resigned sharing her letter of resignation with the Blade.
Taylor Lianne Chandler, a member of the Capital Pride board of directors since 2019 who served as the board’s secretary, submitted a letter of resignation on Feb. 24 that alleges the board has failed to address instances of “sexual misconduct” at Capital Pride.
“This board has made its priorities clear through its actions: protecting a sexual predator matters more than protecting the people who had the courage to come forward. … I have been targeted, bullied, and made to feel like an outsider for doing what any person of integrity would do – telling the truth,” Chandler wrote in her resignation letter.
The Blade reported the organization announced, “As we continue to grow our organization, we’re proactively strengthening the policies and procedures that shape our systems, our infrastructure, and the support we provide to our team and partners.”
Again, it is four months later, and there has been no information from Capital Pride regarding that investigation.
Chandler said a Capital Pride investigation identified one individual implicated in a “pattern” of sexual harassment related behavior over a period of time. She added she was bound by a Non-Disclosure Agreement that applies to all board members and she cannot disclose the name of the person implicated in alleged sexual misconduct or those who came forward to complain about it. She added, “It was one individual, but there was a pattern and a history.”
Again, reading that letter from Chandler and because of the news being full of the Epstein scandal, it makes me want assurances that no organization representing my community will ever think it can cover up issues like this. Capital Pride leadership must be totally transparent.
Capital Pride is a wonderful organization with so many incredible people working and volunteering there. They make our community proud. I never want to see a blemish on the organization. So, I am calling on them to be open and transparent about the investigation they themselves announced, and let the community know what they found, in detail. More important even than the entire community knowing, is for their staff and volunteers to know what they found. No one should be bound by an NDA, which leads to people thinking something really bad is going on.
I thought twice, even three times, before writing this column. I don’t want it to be seen as casting aspersions on all of Capital Pride, or anyone who may have worked there, or volunteered there. But again, because of the focus on the Epstein scandal, and my writing about the felon and his Cabinet officials involved in it, my calling for them to come clean and tell us all they know, I feel compelled to say the same to the organization I have supported over the years, which even honored me as a Capital Pride Hero in 2016. I want them to move forward and be a beacon of light for our community for many years to come. The work they do makes a difference for so many.
I wrote in my memoir that coming to a Pride event helped me to come out, and I am sure it has done the same for so many others in our community. What Capital Pride does is important and it must be as transparent as we demand of any other organization.
Peter Rosenstein is a longtime LGBTQ rights and Democratic Party activist.
Opinions
An undeclared war of distraction by the felon
Will Trump claim a national emergency to undermine midterms?

The president of the United States in his rambling speech about our attack on Iran, recorded during a campaign trip, said, “The Iranian regime seeks to kill. The lives of courageous American heroes may be lost and we may have casualties — that often happens in war — but we’re doing this not for now. We’re doing this for the future, and it is a noble mission.”
Well, the United States has not declared war on Iran, only Congress can do that, not the president. As I write this, the felon has yet to make a live speech to the American people about what he is doing, and Americans have already lost their lives. He is weekending as he usually does at Mar-a-Lago. I wonder if he has the balls to head out to the golf course while American lives continue to be at stake.
This operation is clearly the felon’s way of distracting the people of the United States from his failed domestic policies. From rising food prices, rents, and health insurance. From the loss of manufacturing jobs, as reported in November ”manufacturing shed another 6,000 jobs in September, for a total loss of 58,000 since April.” Had he not acted on Iran now every news outlet in the nation would have reported on the Epstein scandal with the release of the depositions, video and transcripts, of former Secretary of State Hillary Clinton and former President Bill Clinton, in front of the Congressional Oversight Committee.
Even more frightening is this may be his way of preparing to claim a national emergency to undermine the midterm elections, which he is clearly on target to lose, now that his Save America Act has been defeated in Congress.
Americans must ask themselves how long they will put up with this warmonger, racist, sexist, lying, homophobic, SOB, who cares not a whit for them, but only for himself, and his rich colleagues, taking as much grift as they all can, while he is president.
None of this is to say we shouldn’t put constraints on Iran, work to see they never have a nuclear bomb, and limit their production of missiles. We were working toward the goal of stopping them from having a nuclear bomb when the felon, in his first term, pulled us out of the agreement to move forward on that. Today, he has sidelined the State Department, and his Secretary of State, Marco Rubio, in negotiations, and has relied on his son-in-law, Jared Kushner, and Steve Witkoff. The attack was commenced while negotiations were underway. At the end of last week it was reported, Oman’s Foreign Minister Badr Al-Busaidi, who mediated the talks in Geneva, said there had been “significant progress in the negotiation.” Al-Busaidi added, “Technical-level talks would continue next week in Vienna, the home of the International Atomic Energy Agency.” The United Nations’ atomic watchdog likely would be critical in any deal.
So clearly this is all about what the two negotiators, who have sidelined the State Department, Kushner and Witkoff, secretly reported to the felon. My guess is some progress was being made, clearly it was not what the president wanted. So, what ruled was his immediate need for a distraction after the failure of his State of the Union address to make any impact on his sagging poll numbers.
I have written often of the alternate universe Trump has us living in. I am just waiting for his MAGA cult to react to this. Will they still blindly follow everything he says, or will the Laura Loomers of the world finally say, “screw this, take care of us at home, do what you promised to make our lives better”. The first MAGA to say this was Marjorie Taylor Greene. Then Tucker Carlson added his slam against the felon. His PR flack, Karoline Leavitt, is getting confused by all the lies, recently saying “things are better than they were last year.” Clearly forgetting last year was 2025, and the felon was president for all except for 20 days of it, so is responsible for last year.
I am an optimist and believe our democracy will survive him, and his fascist cohorts’ blatant attacks. We won a revolution against one king, and survived a civil war, becoming even stronger as a united nation. We helped Europe defeat Hitler. I believe Sen. Mark Kelly (D-Ariz.) when he says the military will reject illegal orders. Orders that ask them to act against their fellow countrymen and women. I believe the American people will come to their senses before it’s too late. They will finally reject the POS in the White House, and the sycophants, and fascists, surrounding him in time to reclaim our nation for all the people.
Peter Rosenstein is a longtime LGBTQ rights and Democratic Party activist.

I recently lost my dog, Argo.
He was a pit bull, big, sweet, endlessly cuddly, and for 15 years he was my constant. The kind of presence you stop consciously noticing until they’re gone and the quiet hits you all at once. Pit bulls have a reputation. Argo never got the memo. He just loved people, completely and without condition, from the moment he met them until his last day.
I wasn’t prepared for what happened next.
My phone filled up. Instagram lit up. Texts came in from people I hadn’t heard from in months, in some cases years. Hugs from neighbors. Messages from colleagues. Condolences from people I’d lost touch with, some through nothing more than the slow drift of busy lives in a busy city, and some honestly through small tiffs and misunderstandings that neither of us ever bothered to resolve.
And sitting with all of that love pouring in, I found myself asking a question I wasn’t expecting: Why has it taken this long?
We do this in D.C. We get caught in our heads, our calendars, our ambitions. We let weeks turn into months. We let a small misunderstanding calcify into distance because nobody wants to be the first one to reach out, nobody wants to seem like they need something. We perform resilience so well that sometimes the people who care about us most don’t know we need them.
And then something breaks open, a loss, a moment of real vulnerability, and suddenly people show up. And you realize the connection was always there. It just needed permission.
Argo gave people permission. Even in dying, he did what he always did when he was alive. He brought people together.
I’ll be honest with you about where I’ve been lately. As I’ve climbed the entrepreneurial ladder, something quietly shifted. People stopped seeing Gerard. They started seeing a title, a resource, someone who could give them something or who owed them something. A character. Not a person. And when most of your day is spent inside other people’s problems and crises, you can start to feel it, a slow creep of cynicism that you don’t even notice until one day you realize you’ve gone numb.
And I’m not alone in that. Look around. We just watched innocent people die while those in power looked us in the face and called it something else. We watched people erupt over a 10-minute halftime performance like it was the greatest threat to our country. Everywhere you look there is something designed to make you angry, or exhausted, or both. Anger and numbness have become survival strategies. I understand it. I’ve lived it.
But here is what Argo reminded me.
The world is not what the loudest voices say it is. The world is what shows up when something real happens. And what showed up for me, after losing my sweet boy, was people. Caring, loving, present people who put down whatever they were doing to reach out to a friend. Some of them I hadn’t spoken to in too long. Some of them I’d had friction with. All of them showed up anyway.
That is the world. That is what it actually is underneath all the noise.
I think we’ve forgotten that. Or maybe we haven’t forgotten it, maybe we’re just so tired and overstimulated and battle-worn that we’ve stopped letting ourselves feel it. Because feeling it requires vulnerability, and vulnerability feels dangerous right now. It’s easier to scroll. It’s easier to stay mad. It’s easier to keep a wall up and call it wisdom.
Argo spent 15 years showing me a different way. He never met a stranger. He never held a grudge. He never saved his love for people who deserved it on paper. He just gave it, freely, every single time. Not a reward. Not a transaction. Just the most natural thing in the world.
Grief burns off everything that isn’t essential and leaves only what matters. What’s left for me is this: the world is full of good people. You may be surrounded by more of them than you know. And if you’ve gone numb, or angry, or so busy surviving that you’ve stopped connecting, I want you to know that the feeling can come back. It came back for me.
Reach out to someone today. Close a distance you’ve let grow. Tell someone they matter. Not because everything is perfect, but because connection is how we survive when it isn’t. Living disconnected, mad and closed off isn’t living at all. It’s a slower kind of dying.
Death came to teach me how to live. I hope this saves you some time.
Gerard Burley, also known as Coach G, is founder and CEO of Sweat DC.

Man stuck in Lebanon as Iran war escalates

CAMP Rehoboth hires new executive director

Claudia López wins primary in Colombian presidential race

Too afraid to leave home: ICE’s toll on Latino HIV care

Intense doc offers transcendent treatment of queer fetish pioneer

13 HIV/AIDS activists arrested on Capitol Hill

PHOTOS: Sydney Gay and Lesbian Mardi Gras Parade

Fla. Senate passes ‘Anti-Diversity’ bill that could repeal local LGBTQ protections

Ugandan activist named Charles F. Kettering Foundation fellow

Liza Minnelli makes surprise appearance at GLAAD Media Awards
-

 National5 days ago
National5 days ago13 HIV/AIDS activists arrested on Capitol Hill
-
Photos5 days ago
PHOTOS: Sydney Gay and Lesbian Mardi Gras Parade
-
Florida3 days ago
Fla. Senate passes ‘Anti-Diversity’ bill that could repeal local LGBTQ protections
-
Uganda4 days ago
Ugandan activist named Charles F. Kettering Foundation fellow



