News
O’Malley seeks ENDA passage, ban on housing discrimination
Candidate stands at 1 percent among Democratic hopefuls in recent poll


Martin and Katie O’Malley (Washington Blade photo by Michael Key)
Democratic presidential candidate and former Maryland Gov. Martin O’Malley on Monday called for the addition of LGBT employment and housing protections in federal law following the U.S. Supreme Court decision in favor of marriage equality.
“Last week the Supreme Court affirmed that marriage is a human right, and now gay and lesbian couples will be able to marry in every state in our country,” O’Malley said in a statement. “While this is a major step forward, our fight for equality continues. In a majority of states, gay and lesbian employees can still be denied job opportunities or fired solely based on their sexual orientation or gender identity. Twenty-eight states also lack laws banning discrimination in housing.”
O’Malley noted that Maryland law has “long banned” discrimination based on sexual orientation and under his administration last year, he signed into law a measure prohibiting transgender discrimination in the state.
To enshrine into federal law employment protections for LGBT people, O’Malley said Congress should pass the Employment Non-Discrimination Act. The measure hasn’t yet been introduced in 114th Congress, but in years past it has aimed to prohibit employment discrimination in most cases on the basis of sexual orientation and gender identity.
“Passing the Employment Non-Discrimination Act to expand these protections at the federal level is a necessary next step,” O’Malley said. “We must continue to improve our laws, to more fully protect the rights of every individual — and more fully realize the vision of an open, respectful and inclusive nation that Friday’s decision aspires us to be.”
The candidate articulates support for ENDA ahead of the expected introduction of a comprehensive LGBT non-discrimination bill in Congress by Rep. David Cicilline (D-R.I.) and Sen. Jeff Merkley (D-Ore.). Matt Corridini, an O’Malley spokesperson, said his boss is aware of the legislation and supports it.
O’Malley’s competitors for the Democratic nomination for the White House have taken different approaches to the issue of LGBT non-discrimination.
Former Secretary of State Hillary Clinton has called for a ban on discrimination against LGBT people “so they can live, learn, marry, and work just like everybody else.” Although she’s supported ENDA in years past, she hasn’t articulated in this election cycle the best vehicle to achieve non-discrimination protections for LGBT people.
U.S. Sen. Bernard Sanders (I-Vt.) voted for a version of ENDA in 2013. In an interview with the Washington Blade, Sanders said he’d back amending the Civil Rights Act and the Fair Housing Act to include sexual orientation and gender identity and anticipates he’ll support the upcoming comprehensive LGBT bill.
O’Malley faces a significant uphill battle in efforts to win the Democratic nomination for president. According to a Fox News poll, Clinton enjoys 61 percent support among likely Democratic voters nationwide. Sanders follows her with 15 percent support, Vice President Joseph Biden has 11 percent, New York Gov. Andrew Cuomo has 3 percent, former U.S. Sen. Jim Webb has 2 percent and O’Malley has 1 percent.




The Comings & Goings column is about sharing the professional successes of our community. We want to recognize those landing new jobs, new clients for their business, joining boards of organizations and other achievements. Please share your successes with us at [email protected].
Congratulations to Congresswoman Sarah McBride (D-Del.) on being honored with this year’s Stonewall Award from Whitman-Walker Health. Amy Nelson, senior director of Legal Services, said, “Congresswoman Sarah McBride is working to make healthcare accessible to all, and this award recognizes her support of healthcare as a human right. Our legal program supports families facing unprecedented challenges to stay healthy and safe – families that Congresswoman McBride champions with a deep understanding of the issues they face and the legislative expertise of how to support them.”
McBride, in a press release, said, “I am honored to accept this year’s Stonewall Award from Whitman-Walker Health — an organization that has spent 40 years doing vital work to ensure every person can access the dignity of care. In the wealthiest and most developed nation on earth, the ability to receive care should not be a matter of luck—it should be the law of the land. I am proud to be recognized as a partner in this work and to support Whitman-Walker Health in their mission to build a healthier society for all.”
Congratulations also to Wes Drummond who will join Clear Space Theatre Company in Rehoboth Beach, Del., as its third artistic director. Managing Director Joe Gfaller said, “This is an exciting moment of growth for Clear Space as we welcome Wes to join our remarkable team. I am confident he will be an excellent partner as we work with our entire staff, board, and committed team of volunteers, to ensure Clear Space can achieve its full potential in pursuit of our mission to unite and enrich our community through every production on stage, and every arts-based learning program we offer throughout our community.”
On accepting the position Drummond said, “I’m honored to join Clear Space Theatre Company as artistic director, and beyond excited for what we’re about to create together. Clear Space has established itself as a vital and vibrant part of the cultural life of coastal Delaware, and I feel incredibly fortunate to step into this next chapter alongside such a passionate and dedicated team. Rehoboth Beach is a place defined by creativity and community, and I look forward to listening, learning, and building meaningful relationships across the region in the months ahead. My vision is to help Clear Space continue to grow as a bold, forward-thinking, cultural force, that champions fearless storytelling.”

Drummond served in leadership roles at Duluth Playhouse in Duluth, Minn., from 2021 to 2026, including four years as executive director followed by one year as executive producing artistic director, guiding the organization through a period of significant transformation and stability in the wake of the COVID-19 pandemic. As a director, he has worked extensively in New York City, Chicago, and at regional theaters across the country, directing both musical theater and plays with a focus on storytelling that bridges classical works with contemporary perspectives. He has collaborated with leading figures in the industry, including Tony Award-winning director Matthew Warchus, and Tony-nominated director Michael Greif. He is an associate member of the Stage Directors and Choreographers Society.
Wes earned his MFA in directing, Penn State University, where he studied under Tony-nominated director, Susan H. Schulman.
Virginia
Va. Supreme Court invalidates Democrat-backed redistricting plan
Voters narrowly approved new congressional districts last month

The Virginia Supreme Court on Friday struck down a Democrat-backed redistricting plan that voters approved last month.
Ten of 11 of Virginia’s congressional districts favor Democrats in the plan that passed by a 51-48 vote margin in last month’s referendum.
The Human Rights Campaign PAC is among the groups that support it. The court by a 4-3 majority invalidated the referendum results.
District of Columbia
Maren Morris to headline Capital Pride Concert
Grammy award-winning singer/songwriter came out as bisexual in 2024
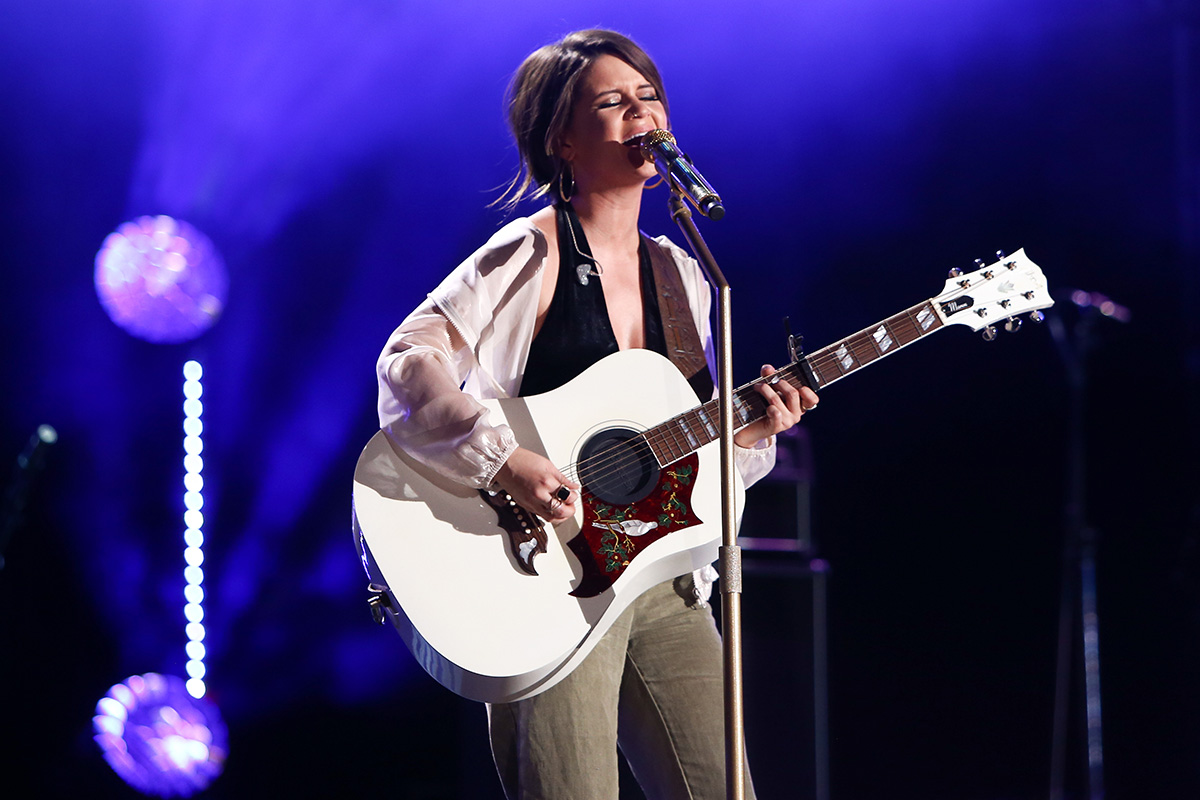
Capital Pride Alliance, the group that organizes D.C.’s annual LGBTQ Pride events, announced on May 7 that nationally acclaimed singer-songwriter Maren Morris, who identifies as bisexual, will be the headline performer at this year’s Capital Pride Concert scheduled for June 21.
The concert takes place as part of the annual Capital Pride Festival held on Pennsylvania Avenue, N.W., usually between 3rd Street near the U.S. Capitol and 9th Street.
“Morris, known for her genre-blending sound and outspoken support of LGBTQ+ rights, will be joined by a standout lineup, including acclaimed queer rapper Leikeli47, pop icon Lisa Lisa, Juno-nominated producer and DJ from the ‘Heated Rivalry’ soundtrack, Harrison, and ‘RuPaul’s Drag Race’ Season 18 winner Myki Meeks,” according to a statement released by Capital Pride.
“In a moment when LGBTQ+ people are being challenged across the country, the Capital Pride Concert is a space where our community is fully seen and heard,” Ryan Bos, the Capital Pride Alliance CEO and president, said in the statement. “Bringing Maren Morris to the stage reflects this year’s theme: Exist, Resist, Have the Audacity,” Bos said.
The statement notes that the concert takes place as part of the annual D.C. Pride Festival, which is open to the public free of charge, with tickets available for purchase for specific areas listed as the Capital Stage Pit Zone and the VIP Concert Zone.
It says the festival takes place from 12 –10 p.m. and points out that in addition to the music performed by multiple other performers on several stages, festival attendees “can explore hundreds of exhibitors, community organizations, and artisans, along with multiple food courts and beverage gardens throughout the festival footprint.”
Information on the Capital Pride Alliance website shows that the festival takes place one day after the annual Capital Pride Parade, scheduled for June 20 and which is expected to travel from 14th and T Streets, N.W., to Pennsylvania Ave., N.W., where it is expected to end at 9th Street.
The statement adds that following the stage performances during the June 21 festival, which are expected to conclude around 8 p.m., “the celebration will continue with the Capitol Sunset Dance Party, closing out the evening against the backdrop of the U.S. Capitol.”
The online publication Today, which is part of the NBC “Today” television show, reported that Morris came out as bisexual in a 2024 during Pride. It reports Morris “shared several images of herself holding a Pride flag to mark the occasion, writing, ‘Happy to be the B in LGBTQ+’”

Comings & Goings

Learn more about queer love

Calendar: May 8-14

Va. Supreme Court invalidates Democrat-backed redistricting plan

Maren Morris to headline Capital Pride Concert

Under new extremism laws, LGBTQ Russians must fight to survive

How do you vote a child out of their future?

Gay ICE detainee freed after 150 days in detention

A reign defined by commitment and human impact




