Opinions
Lessons for D.C. from my husband’s painful death
City Council should embrace Dignity Act


Sean Sasser (Washington Blade file photo by Michael Key)
My late husband, Sean Sasser, taught a whole generation of Americans what it’s like to be a person of color, gay and living with HIV. Back in 1994, he was a fixture in MTV’s “Real World: San Francisco” household, and his public advocacy for people living with HIV was revolutionary. Sean was a natural educator and activist, and I know that if he were alive today, he would be supporting the D.C. Death with Dignity Act.
The dying process that Sean endured is a case study in why we need this law, which would authorize medical aid in dying and allow terminally ill adults to get a prescription they can take, when and if they decide, to end unbearable suffering in their final days or weeks.
Sean was a dynamic, loving man. He was a mentor to several kids, a pastry chef with 12 staff and two restaurants under his management, and for a time, a co-parent with me to our foster daughter Alice.
Sean was a big guy, a strong guy, a man with presence; but in 2013, he began losing weight, feeling exhausted and experiencing pain. Within less than a few months, he was diagnosed with stage 4 Mesothelioma, a diagnosis most often followed by less than 12 months to live.
Sean was determined to fight the cancer. He sought chemo, and any advice he could get. Even after his oncologist thought it was time to move toward hospice, Sean wanted to push forward with treatments. And so we did.
Eventually, however, the time came when Sean could barely get himself out of bed and to the bathroom. His pain was excruciating, and it landed him in the emergency room three times in one month. The oncologist could see no path forward; Sean had become too weak to even continue chemo.
I wish I could say that his decision to accept his inevitable death and enter hospice brought him peace, but it did not. The pain only got worse as we waited for the inevitable. I recall weeks before he passed, his emaciated body still persevering, him saying, “Why is this taking so long, I want it to be over already.”
And to be frank, so did I.
This once strong man, who could lift our foster daughter under one arm and our goddaughter under the other, was now not even able to roll over or use a bedpan. Even for the most basic of needs, he was dependent on me.
As skilled and compassionate as his hospice team was, I will always be angry that we did not have more options to help Sean get past the suffering.
My husband was ready to let go and be done with the pain and long farewell. But here in D.C., his only choice was to endure the terror, the powerlessness and pain. My only choice was to try to help him through it, to simply wait for the inevitable as he suffered needlessly.
Sean’s drawn-out dying process reminded me of days gone by, in the field both of us worked, when people dealing with AIDS had no treatment options and suffered drawn out, painful deaths.
In fact, it was AIDS that helped inspire a more human response for so many. The mothers, lovers and friends of people dying the uniquely agonizing death that AIDS once wrought petitioned lawmakers for better, more merciful options. Oregon was the first state to adopt a law, and for nearly 20 years, that state’s health department has documented that it has worked exactly as intended, giving peace of mind to countless people facing a terminal illness, and their loved ones. Washington State, Montana, Vermont and California also give their adult residents, who are mentally capable and have less than six months to live, this same option.
It is unacceptable to me that here in Washington, D.C., we can’t allow mentally capable adults like my husband the option of aid in dying when death is a certainty, why we can’t let them go gracefully, with dignity, and peace. Why are we forced to wait in pain — physical pain for the patient, emotional pain for the family – while a punishing dying process plays out?
Members of the D.C. Council and Mayor Bowser will soon be deciding whether to give us the choice – when there is no hope for a cure and palliative care cannot comfort – to get a prescription that lets us die peacefully in our sleep. It’s what Sean would have wanted, and our leaders have no right to deny us this compassionate end-of-life option.
Michael Kaplan is former CEO of AIDS United.






Opinions
A vice president marches by our side
New exhibit explores Pride in the 2020s and asks what’s to come
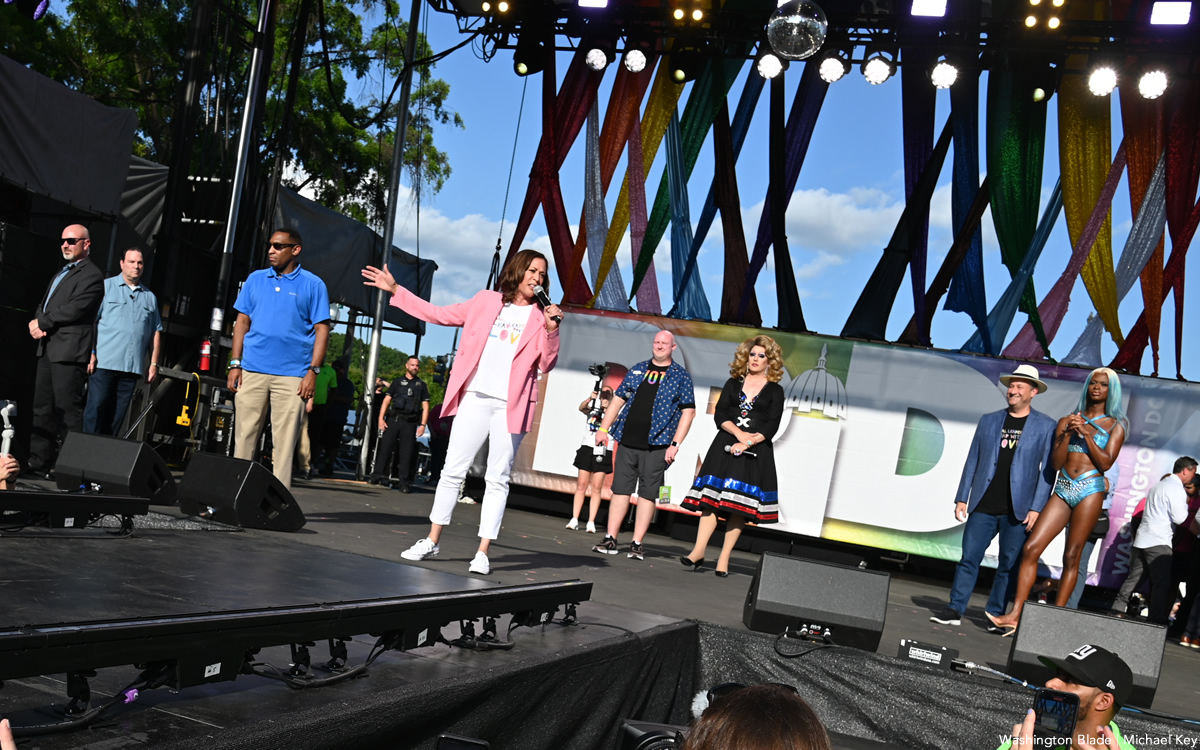
A photograph can change how we understand ourselves. In Rainbow History Project’s exhibit “Pickets, Protests, and Parades: The History of Gay Pride in Washington,” one pairing does exactly that: 10 Washingtonians in their Sunday best picketing the White House in 1965, and, a few panels later, Vice President Kamala Harris in a “Love is Love” Tshirt marching down Pennsylvania Avenue for Capital Pride in 2021. Between those two moments—anxious, buttonedup defiance on one side of the White House fence and a sitting vice president cheering among rainbow flags on the other—lies the story this exhibit tells.
Last year, we stretched that story along Freedom Plaza for WorldPride 2025, just three blocks from the White House. Over seven weeks, visitors from around the globe walked a timeline that showed how a small, risky White House picket helped ignite six decades of increasingly visible, intersectional Pride in the nation’s capital. They met organizers who insisted that gay history did not start at Stonewall, and that D.C. has been a laboratory for LGBTQ resistance since at least that first 1965 picket.
This June, as part of Dupont Underground’s “Matters of Pride” programming, we’re inviting you back underground to revisit what we showed the world last year—and to look harder at what it asks of us now. The tunnels below Dupont Circle will host the early eras of the exhibition: the White House picket; block parties at Lambda Rising bookstore, the first National March for Lesbian and Gay Rights in 1979 that brought more than 100,000 people onto the Mall; and the first D.C. Pride march that began at Howard University, led by BIPOC activists who carried every part of their identities into the streets.
Seen together, these moments make the theme “A Vice President Marches By Our Side” less about a single VIP participant and more about a changing relationship between our movements and the state. In 1965, picketers carefully followed dress codes to appear “employable” enough to be heard at all. By 1979, marchers filled the National Mall with banners that linked sexuality to feminism, racial justice, and antiwar activism. By the 2020s, a vice president could show up at Capital Pride, call for the Equality Act, and speak explicitly about protecting trans youth and communities of color. None of those shifts were guaranteed. All of them were built, step by step, by people who kept organizing whether or not anyone in power joined them.
The reinstall is also a chance to notice details you may have rushed past on a crowded WorldPride weekend: a handlettered sign demanding federal jobs in 1965; a quote from a 1970s organizer about the sheer relief of dancing in public; a photograph of local pioneers like SaVanna Wanzer, the founder of D.C. Trans Pride and Black Trans Pride, whose work helped make today’s Pride more fully trans inclusive even as Black trans folx remain under attack. These are not just artifacts; they are reminders of how much was risked so that we could take Pride for granted at all.
We are reinstalling this exhibit at a moment when very little about the future feels guaranteed. America’s 250th birthday is around the corner, and national debates over whose stories “belong” in the classroom, the public square, or in the archives, are already shaping policy. In that context, going back to the origins of D.C. Pride is more than nostalgia. It is a strategy lesson. The 1960s picketers, the 1979 marchers, the BIPOC activists leaving an intersectionality conference at Howard and marching to the Mall—all of them faced hostile climates, limited resources, and no certainty of success. Yet they showed up anyway, and in doing so, they expanded what was imaginable.
That is why, at the end of the reinstall, the exhibit turns back on you. The final section, “The Next 60 Years of Pride,” remains intentionally unwritten. Instead, you will find a simple question on the wall: “What will you do?” Visitors will have the chance to add their own commitments—large or small—to the story: what they will march for, organize for, or quietly sustain in the years ahead.
A vice president once marched by our side. This month at Dupont Underground, we are asking something both humbler and more radical: after everything we have learned from the past six decades of Pride in Washington, who will you be standing with, and what will you be brave enough to do next?
In conjunction with WorldPride 2025 the Rainbow History Project exhibited “Pickets, Protests, and Parades: The History of Gay Pride in Washington.” More than two years of planning resulted in seven weeks of outdoor education, centering the voices of Pride’s organizers. In the final of the 10 themes, we discuss “A Vice President Marches By Our Side,” about what Pride looked like in the 2020s and asking about Pride in the years to come.
Vincent Slatt volunteers as the senior curator at the Rainbow History Project.
Opinions
Leaving for a barge trip through canals of Burgundy
Nervous about European reactions to Americans given Trump’s war in Iran

As those who read my columns know, I love cruising, the kind you do on water. I have had many different cruise experiences, including sailing through the Galapagos and the Norwegian fjords. This time, I will be doing something a little different and am off on a new adventure. With 18 others, will be on a barge for six days, going from Lyon to Paris, through the canals of Burgundy. Each day will bring a new adventure. We will be embarking in Besancon, and traveling to Beaune, Arc-et-Senans, Dole, Saint-Jean-De-Losne, Seurre, Chalon-Sur-Saone, and then disembarking in Auxerre, en route to Paris. Of the 18 people, four are friends from D.C. and Rehoboth Beach. I look forward to meeting the other travelers.
I leave for Paris on June 8 and made arrangements for a car in Paris to take me to the Gare De Lyon, to board a fast train to Lyon. A quick two-hour trip. In Lyon I will head to the hotel for a welcome dinner, where I will meet our guide and other travelers. This is a Gate 1 adventure booked by my friends at My Lux Cruise. We will be spending two days in Lyon before boarding the MS Daniele, built in 2016. It is modern, with space for both indoor and outdoor dining, a small lounge, the requisite bar, and very simple staterooms. Mine will have two single beds. Can’t forget the hot tub on the bow. I will be writing a blog during my trip, which will be published in the Blade, likely after my return. I will post pictures during the trip on social media. After six days on the barge, we arrive in Paris, where I will spend a couple of days with good friends. One planned excursion is to see the rebuilt Notre Dame.
I will be away from D.C. on June 16, primary day. Since for the first time there will be ranked choice voting, it is possible we won’t know who wins until I get back on June 19. I hope everyone votes, and urge you to vote, as I already have, for Kenyan McDuffie for mayor. His main opponent, Janeese Lewis George, clearly doesn’t understand how D.C. government really works. She is trying to emulate NYC Mayor Mamdani with promises, but hers won’t happen. We don’t have a governor, and state legislature, to help. Our governor is in essence the felon in the White House, and our state legislature is the Congress. They won’t be helping. In addition, George has claimed the endorsement of an antisemitic organization, DSA, and is going to birthday parties for a guy who calls gay men like me ‘fags’ and says they shouldn’t be teaching his children in the public schools. The winners of the Democratic primary races will determine how D.C. moves forward. It really makes a difference.
The world is a different place today than it was just a short 18 months ago, when the felon began his second term. This is the first time I will be out of the country since he began this illegal war with Iran, plunging the world into chaos. I wonder what the reception for an American will be in Europe these days. I remember back when Ronald Reagan was first elected, which was the last time in my travels, before Trump, I felt compelled to apologize for my country. At that time people would actually come up to me and ask, what did America do, and why? Yet as bad as times seemed then, they were nowhere as bad as they are today. The felon in the White House has made life so much worse for people around the world. Europeans have seen him get on his knees to Putin, and screw Ukraine. Now with this illegal, and unnecessary, war in Iran, he is impacting their lives directly. Fuel prices are rising dramatically, and there is a drastic shortage of jet fuel, causing cuts in flights. They see him work hand-in-hand with the war criminal, Netanyahu, in Israel. They see how he simply wants to enrich himself with things like his ‘Board of Peace,’ and in the long run, screw the Palestinian people. It will be interesting to hear how Europeans feel about all this. I look forward to listening to them. All I can say in response is I didn’t vote for Trump and will continue to demonstrate, and write against him, as often as I can.
Putting politics aside, which is hard to do these days, I am excited about this new adventure, and look forward to sharing some of my experiences with you.
Peter Rosenstein is a longtime LGBTQ rights and Democratic Party activist.
Opinions
Barney Frank’s powerful legacy for LGBTQ federal employees
The ‘Great Gay Communicator’ deserves respect

Former Congressman Barney Frank, who died last week, was dogged during his life over being gay. The self-proclaimed only “left-handed, gay, Jewish congressman,” in Congress deserved better.
Frank’s perseverance paved the way for others. With wit and intelligence, he helped educate Americans about sexuality. As a federal employee and a member of the Federal Gay, Lesbian or Bisexual Employees (GLOBE), a government-wide organization founded by Dr. Len Hirsch, I saw Frank’s unforgettable speaking style when he was a guest speaker at our monthly events.
Frank’s detailed presentations about federal employment policies were not recorded. The only record of them, edited by Dr. Hirsch and other members of the GLOBE board, is in the minutes of the GLOBE meetings. I held several positions in GLOBE, including secretary, assistant newsletter editor, and as an elected member of the board. I drafted the minutes of the meetings.
GLOBE’s minutes were edited to protect the identity of federal employees. This was important because then-U.S. Sen. Jesse Helms (R-N.C.) attempted to obtain the minutes. Helms felt LGBT advocacy in the federal workplace was an illegal form of political activity. GLOBE was also concerned that the minutes would be illegally accessed and forwarded to Helms or used to blackmail federal employees. GLOBE’s minutes are preserved at the National Archives.
When I was named Gay, Lesbian, Bisexual Program Manager at the Department of Agriculture in 1993, I immediately notified Frank’s office of my appointment. After a federal newsletter published an article about a speech I gave, Helms accused me of using government resources to support “a homosexual agenda.” During several hours on the evening of July 19, 1994, Helms told the Senate and C-SPAN’s television audience that LGBT federal employees had their minds in their crotches. He called LGBT federal employees “perverts.”
Helms had government documents that described the position of “Gay, Lesbian, Bisexual Program Manager.” It was a program that used the incendiary words “promote” and “recruit” homosexuals. It was a huge mistake for government bureaucrats to have written such a program. Helms published it in the Congressional Record. Frank helped us through this battle and others.
Aside from Frank, there were other LGBT members of Congress in the 1990s. Gerry Studds (D-Mass.), Steve Gunderson (R-Wisc.), and James Kolbe (R-Ariz.). Studds was censured for an affair with a 17-year-old male page in the House. Gunderson was publicly outed by a fellow House Republican. Kolbe was subject to sexual accusations.
Among these gay congressmen, Frank weathered a hostile media, personal scandal, and vicious attacks from his Republican colleagues. In 1995, former Texas GOP House Majority Leader Dick Armey was caught referring to Frank as “Barney Fag.” His apology was grudging.
“I rule out that it was an innocent mispronunciation,” responded Frank. “I turned to my own expert, my mother, who reports that in 59 years of marriage, no one ever introduced her as Elsie Fag.”
After celebrating his 72nd birthday, Frank married his longtime partner. He successfully worked to place marriage equality into the 2012 Democratic platform, which President Obama endorsed.
Still, Frank was dogged by homophobia. The Tea Party’s Doug Mainwaring called Frank’s wedding “a mockery, a parody, a staggering caricature of the most fundamental and towering of American institutions.”
In an interview with Washingtonian magazine, Frank said he “hates being classified as ‘the gay congressman,’” as his legislative accomplishments go beyond gay rights. He co-sponsored the 2010 Dodd-Frank Wall Street Reform and Consumer Protection Act.
Frank will especially be remembered in Washington for his sharp wit. He once referred to advocating for gay marriage legalization as “cruising for gay rights.” He wrote devastatingly funny op-ed pieces, notably for the Washington Post.
Though Frank may not have wanted to be known as a gay congressman, when he spoke, the LGBT community listened. He was the Great Gay Communicator. Barney Frank deserved respect. May his memory be a blessing.
James Patterson, a life member of the American Foreign Service Association, is a writer and communications consultant in the D.C. area.

PHOTOS: Fairfax City Pride

EXCLUSIVE: Pelosi reflects on four decades of LGBTQ advocacy

D.C. prepares to party as Pride celebrations kick off Saturday

David Archuleta, Monroe Alise named D.C. Pride parade marshals