News
Gay former U.S. ambassador drops congressional bid


Gay U.S. ambassador Daniel Baerhas dropped his congressional campaign. (Washington Blade photo by Michael Key).
A gay foreign policy expert who worked on international LGBT rights and served as U.S. ambassador to the Organization for Security & Cooperation in Europe has dropped his short-lived bid for a congressional seat in Colorado.
Daniel Baer, who had sought the Democratic nomination to run in Colorado’s 7th congressional district, announced in a statement Thursday he’d suspend his campaign in the aftermath of incumbent Rep. Ed Perlmutter (D-Colo.) deciding to run for re-election.
“When Ed Perlmutter decided to re-enter the race, I took time to reflect on how to move forward,” Baer said. “Running against Ed wasn’t the race I had planned; but while the race had changed, my reasons for running had not. In the end I concluded that while there would be purpose in continuing my campaign, it was less clear that there was wisdom in doing so.”
Baer had declared his candidacy in August for the congressional seat after Perlmutter, a six-term member of Congress, announced he’d retire Congress. Initially, Perlmutter had sought to become governor of Colorado, but dropped that campaign. (Rep. Jared Polis, a gay lawmaker, is still in the Colorado gubernatorial race). Weeks later in August, Perlmutter announced he’d, in fact, seek re-election to Congress.
“Ed works hard to stay connected to folks in our community and he clearly loves being our representative,” Baer said. “I’ll work hard to get Ed re-elected. I’ll send him a check, sign up to knock on doors, and urge my friends to vote for him. I hope everyone else will too.”
Under the Obama administration, Baer served not only as U.S. envoy to OSCE, but deputy assistant secretary of state for the Bureau of Democracy, Human Rights & Labor, where his portfolio included LGBT international human rights issues. After his appointment as U.S. ambassador, Special Envoy for the Human Rights of LGBTI Persons Randy Berry took over the LGBT portfolio at the State Department.
Baer was one of a record number of openly LGBT congressional candidates seeking election ahead of the 2018 midterm election. Other LGBT candidates of note are Maryland State Sen. Rich Madeleno, who seeking to become governor of Maryland; Sen. Tammy Baldwin (D-Wis.), who’s seeking re-election in Wisconsin; and Rep. Kyrsten Sinema (D-Ariz.), who’s running for U.S. Senate in Arizona.






Germany
German group slams White House’s LGBTQ rights record ahead of World Cup
LSVD says trans, nonbinary soccer fans safety ‘not guaranteed’ in US

A German advocacy group on the eve of the 2026 World Cup sharply criticized the Trump-Vance administration over its anti-LGBTQ policies.
The World Cup will take place in the U.S., Canada, and Mexico through July 19. The tournament began on Thursday in Mexico City with Mexico beating South Africa 2-0.
“In the USA, democracy is being gradually dismantled,” said Julia Monro of Federation Queer Diversity, a German LGBTQ and intersex rights group known by the acronym LSVD, in a statement released on Wednesday. “In particular, the human rights of trans, intersex, and nonbinary individuals, as well as other queer people, are facing massive attacks and political instrumentalization by the Trump administration.”
The LSVD statement notes sports “has a special responsibility in this situation because it conveys values worldwide that extend beyond the playing field: fairness, respect, and inclusion.”
“This must apply to everyone, including trans* and nonbinary people,” says LSVD. “Those who love sport must also protect those who can only experience it under difficult circumstances.”
“The public visibility of queer people is being pushed back, companies and organizations with diversity strategies are being pressured, and laws for trans*, intersex, and nonbinary people are being tightened,” added the group. “This is not a fringe issue, but directly affects everyday life, mobility, and safety. The way minority rights are treated is a measure of the state of a democratic society. Inhumane measures must not be normalized. The international community must not remain silent as attention on the host country, the USA, increases. The Trump administration could exploit this media platform for further inhumane purposes, in order to transfer its homophobic agenda to other countries.”
LSVD also stressed the “safety of trans* and nonbinary soccer fans is currently not guaranteed in the USA.”
“We advise all queer fans to inform themselves carefully beforehand and to take precautions for their safety,” it said.
The Council for Global Equality is one of the more than 100 organizations that issued a travel advisory for the U.S. ahead of the World Cup.
LSVD in its statement pointed out the German government in 2025 issued a travel advisory for trans and nonbinary people who are planning to visit the U.S. The warning specifically noted President Donald Trump’s executive order that banned the State Department from issuing passports with “X” gender markers.
InterPride, the organization that coordinates WorldPride events, issued a travel advisory for trans and nonbinary people who planned to travel to the U.S. for WorldPride that took place last summer in D.C.
“Due to an executive order issued by the U.S. president on Jan. 20, all travelers must select either ‘male’ or ‘female’ when applying for entry or visas. The gender listed at birth will be considered valid,” read the InterPride advisory. “If your passport has ‘X’ as a gender marker or differs from your birth-assigned gender, we strongly recommend contacting the U.S. diplomatic mission before traveling to confirm entry requirements.”
LSVD notes the German government reiterated its 2025 travel advisory ahead of the World Cup.
“Anyone traveling with a different gender entry, with an ‘X’ marker in their passport, or who does not conform to the state’s expectations during checks, must expect problems in the USA,” said LSVD.
Virginia
Gay 1920s-era Hollywood star to be honored in Staunton, Va.
Billy Haines became acclaimed designer after anti-gay policies ended his acting career
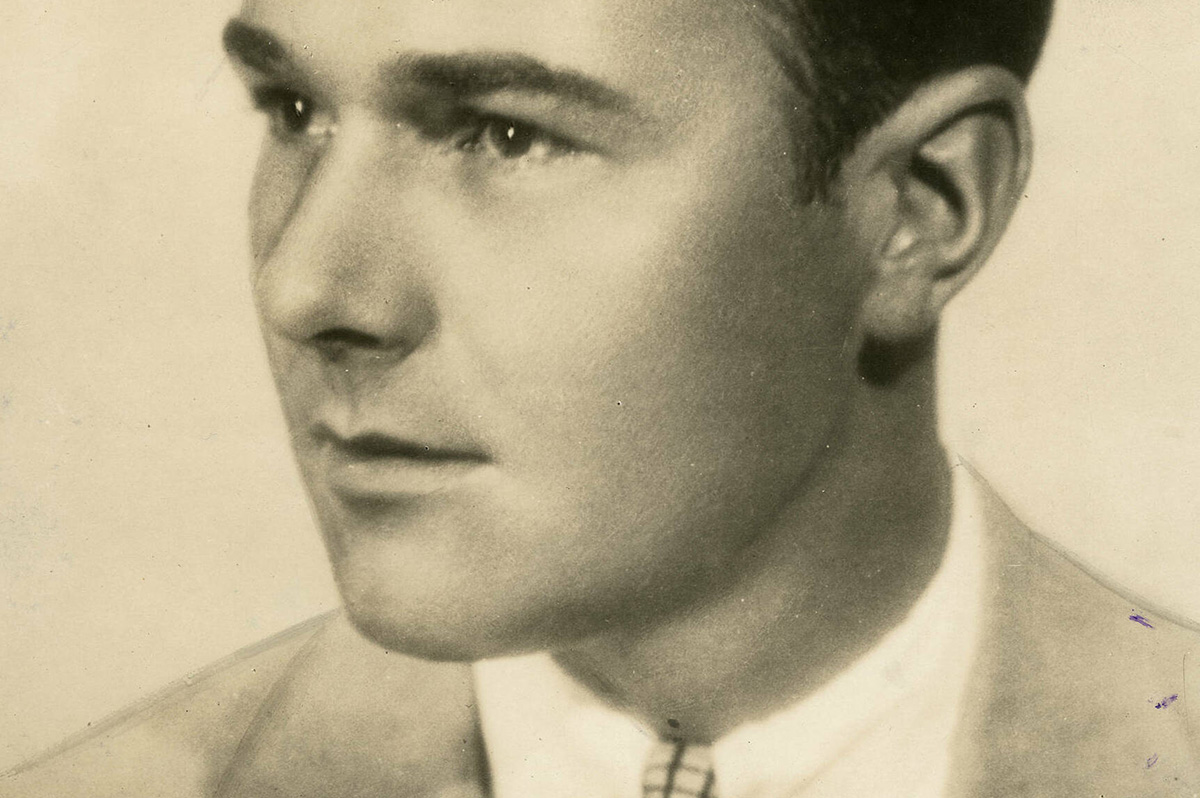
A project is underway in Staunton, Va., to honor William ‘Billy’ Haines, who was born and raised in Staunton before becoming an out gay 1920s and early 1930s-era Hollywood movie star whose acting career ended around 1934 when he refused demands that he conceal his sexual orientation and end his relationship with his male partner.
Haines left the movie business around that time to start what became a highly successful interior design and furniture business in Los Angeles that he led until his death in 1972 at age 72, and which remains in business today, according to the Arcadia Project, a Staunton-based nonprofit initiative.
In a statement released last month, Arcadia Project announced it is working to revitalize a long-vacant movie theater in downtown Staunton that it plans to rename after Haines. It says a fundraising campaign is under way to support efforts to reopen the theater and the larger building in which it is housed as a “dynamic mixed-use cultural center.”
The statement notes that Haines left Staunton at age 14 and resided in Hopewell, Va., and Greenwich Village in New York City until 1922, when he was “discovered” by a talent scout and sent to Hollywood.
“Between 1922 and 1934, Haines appeared in 54 movies during his meteoric and highly successful career,” the Arcadia Project statement continues, noting he transitioned from silent movies to talkies and was fully open about being gay. “But when Hollywood’s moral crackdown of the 1930s demanded that he end his relationship with his longtime partner Jimmie Shields, Haines refused,” it says.
“For LGBTQ people – then and now – Haines’s choice resonates deeply. Rather than deny who he was, he reinvented himself as an interior designer to the stars,” according to the statement.
It says he helped invent the so-called Hollywood Regency style home and designed homes for Hollywood legends such as Joan Crawford, Gloria Swanson, Carole Lombard, George Cukor, and Jack Warner as well as for political figures like Ronald Reagan when he was governor of California.
“As there is no monument, marker or public recognition for Haines in his hometown of Staunton, Va., Arcadia Project, in collaboration with the LGBTQ+ community in Staunton seeks to commemorate him inside a new cultural center,” the statement says.
It quotes Arcadia Project Executive Director Pamela Mason Wagner as saying, “Naming the movie theater in Haines’ honor is more than an act of historical recognition – it is a powerful statement about visibility, belonging, and whose stories are valued in our community.”
The statement says project leaders hope to open the cultural center in early 2027, with a fundraising campaign seeking to raise $250,000 to renovate the theater.
“If the full goal is not reached, a smaller space within the building will be named for Haines, scaled to the amount of funds raised,” it says. “We truly hope friends and admirers of Billy Haines everywhere will want to participate.”
Donations for the project can be made through this site: www.thearcadiaproject.org
District of Columbia
Your queer D.C. voting guide
June 16 primary nears; Lewis George, McDuffie lead in polling for mayor

LGBTQ voters in the nation’s capital are choosing among a long list of LGBTQ supportive candidates running for mayor, D.C. City Council, and the position of D.C. Delegate to the U.S. House of Representatives in the city’s June 16 primary election.
LGBTQ activists who have spoken to the Washington Blade appear to be divided in their support for the two leading Democratic candidates for mayor – D.C. Council member Janeese Lewis George (D-Ward 4) and former D.C. Council member Kenyan McDuffie (I-At-Large) in a seven-candidate race.
Among the other five Democratic mayoral candidates is Rini Sampath, a cyber security consultant who told the Blade she identifies as queer.
“We’re living in an extremely diverse community, an extremely unique community,” she told the Blade. “And being able to self-label, self-identify as queer is something that I just want to take pride in.”
But a poll conducted by the Washington Post and George Mason University’s School of Policy and Government released on June 5 shows Sampath receiving just 3 percent in a sample of likely voters in the D.C. Democratic primary.
The poll, conducted from May 27-June 1, shows Lewis George leading in the mayoral primary with 36 percent compared to McDuffie, who had 25 percent. However, 25 percent of those polled were undecided in the mayoral race, according to the Post, indicating at least some of the undecided voters could go to McDuffie.
“Undecided voters are concentrated among groups that lean toward McDuffie, including moderates, Black voters and those ages 65 and older,” the Post story reporting on the poll states.
Another factor making it more difficult to predict the election outcome is the start in this year’s D.C. primary of ranked choice voting, which enables voters to select as many as five candidates on their ballot as their first through fifth choice depending on how many candidates are running for a specific office, including the office of mayor.
The ranked choice process takes effect if no candidate receives at least 50 percent of the vote in a race with three or more candidates and serves as an instant run-off using voters’ second-choice or third or more choice votes until one candidate receives 50 percent of the vote.
In what appears to support the belief of many local political observers that Lewis George and McDuffie are the two leading mayoral candidates, the poll shows the remaining candidates receiving less than 5 percent.
They include former D.C. Council member Vincent Orange with 4 percent, local real estate manager and developer Gary Goodweather with 3 percent, and former U.S. Department of Homeland Security contractor Hope Solomon and real estate broker and Ward 1 community activist Ernest Johnson each receiving 1 percent.
Goodweather, a political newcomer, has attended LGBTQ events in his mayoral campaign and has expressed strong support on LGBTQ issues.
With that as a backdrop, the Capital Stonewall Democrats, the city’s largest LGBTQ political group, has endorsed Lewis George for mayor and GLAA DC, formerly known as the Gay and Lesbian Activists Alliance of Washington, awarded Lewis George its highest candidate rating score of +10.
GLAA said it did not issue a rating for McDuffie because his campaign did not return a GLAA candidate questionnaire on which it bases its ratings. A spokesperson for the McDuffie campaign said campaign workers later discovered the questionnaire landed in the spam folder of their email account and McDuffie would have returned it had he received it.
At GLAA’s invitation, McDuffie completed the questionnaire and GLAA has posted it with its full responses to a list of 10 questions on the GLAA website along with the questionnaire responses from other candidates, including Lewis George. Like Lewis George, McDuffie expressed strong support for a wide range of LGBTQ issues in his responses, but GLAA said it could not issue a rating for him due to the missed deadline for submitting the questionnaire.
According to GLAA, just two other mayoral candidates returned the questionnaire and received a rating. Sampath received a +6.5 rating, and Johnson received a rating of +4.5. Under the GLAA rating system, a -10 is the lowest possible rating, with a +10 being the highest.
D.C. Board of Elections records show that no Republican candidate is running for mayor and one Statehood Green Party candidate – Robert L. Gross – is running unopposed on the primary ballot for voters registered as Statehood Green Party members. GLAA’s website shows Gross did not receive a rating under the group’s policy of not rating candidates that do not return the questionnaire.
The Statehood Green Party and its candidates for local D.C. offices have historically been supportive of LGBTQ rights.
LGBTQ activists who are backing Lewis George or McDuffie appear to be gravitating to the two based on their political leadings separate from LGBTQ issues, just like voters in general. Lewis George, who identifies as a Democratic Socialist, is popular among progressive voters.
McDuffie, who is seen as a more moderate candidate like current D.C. Mayor Muriel Bowser, is being supported by LGBTQ activists who hold those views, some of whom currently work in the Bowser administration.
Among Lewis George’s LGBTQ supporters are longtime Ward 8 community leader Phillip Pannell and former Capital Stonewall Democrats President Howard Garrett. Among the LGBTQ McDuffie backers are longtime D.C. Democratic activists John Fanning and David Meadows.
“The rights of LGBTQ residents in our country are under attack,” Pannell told the Blade. “We need a mayor of our nation’s capital who will be a progressive voice and force in standing up for our rights and advancing the quality of life for our community,” he said. “That is one of the reasons I enthusiastically support Janeese Lewis George for mayor.”
Fanning, a member of the staff of D.C. Council member Anita Bonds (D-At-Large), said he has observed McDuffie’s work on the Council firsthand. “He has been out and upfront on many of our issues and he has been an ally to our community,” Fanning said. “And I feel more comfortable with his judgements when it comes to city policy,” Fanning said, adding, “And I sense he has more of a pulse on how to grow our economy.”
In the race for D.C. Delegate to the U.S. House, five Democrats are competing in the June 16 primary, including D.C. Council members Brooke Pinto (D-Ward 2) and Robert White (D-At-Large). Pinto and White have been outspoken supporters of the LGBTQ community. Capital Stonewall Democrats has endorsed White.
Also running as Democrats for the congressional seat are community activists Kinney Zalesne, Trent Holbrook, and Greg Jaczko, who have expressed support for LGBTQ issues at candidate forums. Denise Rosado is running unopposed for the congressional seat as a Republican, and Kymone Freeman is running unopposed as a Statehood Green Party candidate in the primary.
Under D.C.’s “closed” primary system voters can only vote for a candidate for a specific political party if they are registered members of that party in the primary. In the general election in November, voters can vote for any candidate regardless of party affiliation.
GLAA has said it does not issue candidate ratings for the D.C. Delegate position, which has been held for many years by Democratic incumbent Eleanor Holmes Norton, who announced earlier this year that she is retiring and not running for re-election. Norton has been a longtime outspoken LGBTQ rights supporter.
D.C. Council Chair Phil Mendelson (D-At Large), also a longtime LGBTQ rights supporter, is running unopposed for re-election in the Democratic primary, He received the Capital Stonewall Democrats endorsement and a +6.5 rating from GLAA.
Nine Democrats are running for the At-Large D.C. Council seat currently held by Bonds, who is also retiring and not running for re-election. Capital Stonewall Democrats has endorsed local pharmacist, community activist, and LGBTQ ally Oye Owolewa, who received a +9 rating from GLAA.
The other Democrats running for the at-large seat who received a rating from GLAA include Lisa Raymond, +7.5; Dwight Davis, +6.5; Dyana Forester, +6; and Fred Hill, +5.5.
Board of Elections ballot records show that Darrell Green is running unopposed for the at-large seat in the Republican Primary and Darryl Moch is running unopposed in the primary as a Statehood Green Party candidate.
In the Ward 1 D.C. Council race, five LGBTQ supportive candidates are competing in the Democratic primary, including two LGBTQ candidates – gay rights activist Miguel Trindade Deramo and bi candidate Aparna Raj. The Ward 1 seat became vacant when incumbent Democrat Brianne Nadeau announced she was not running for re-election.
Capital Stonewall Democrats announced it did not make an endorsement in the Ward 1 race because the endorsement vote by its members was divided and none of the candidates received a required 60 percent of the vote for an endorsement.
GLAA awarded its highest +10 rating to both Deramo and Raj as well as to Ward 1 Democratic candidate Rashida Brown. It assigned a rating of +5.5 to candidate Terry Lynch but did not issue a rating for the fifth Democratic candidate – Jackie Reyes Yanes, who did not return the GLAA questionnaire.
The group didn’t issue ratings for Ward 1 Republican candidate Jett James Jasper or Statehood Green Party candidate Jude Cranniitch, both of whom are running unopposed. GLAA has said it sent out its questionnaire to all candidates listed by the Board of Elections to be placed on the ballot and does not rate those who do not return the questionnaire.
In the Ward 3 D.C. Council race, incumbent Council member Matthew Fruman (D), also an outspoken LGBTQ rights supporter, is running unopposed in the Democratic primary, with no GOP or Statehood Green Party candidate running in the primary. Fruman received the Capital Stonewall Democrats endorsement but was not rated by GLAA.
In the Ward 5 Council race, incumbent Zachary Parker, the Council’s only gay member, is being challenged by two Democrats in the primary – community activists Bernita Carmichael and Bridget French. Parker received the Capital Stonewall Democrats endorsement and a +7 rating from GLAA. Carmichael and French did not receive a GLAA rating.

Political observers in the ward believe Parker is the favorite to win the primary as well as the general election in November, when he will be challenged by Republican Jeffrey Kihien-Palza and Statehood Green Party candidate Joyce Robinson-Paul, who are running unopposed in their party primaries on June 16.
In Ward 6, incumbent Council member Charles Allen (D). a longtime LGBTQ rights supporter, received the Capital Stonewall Democrats endorsement and a +6.75 rating from GLAA. He is being challenged in the primary by Democrats Gloria Ann Nauden and Michael Murphy. Ward 6 political observers consider Allen the strong favorite to win the primary and the general election, when he will be challenged by Republican Jorge Rice, who is running unopposed in the GOP primary. No Statehood Green Party candidate is running for the Ward 6 Council seat.
Capital Stonewall Democrats did not make an endorsement for the D.C. Council special election for the At-Large Council seat that became vacant when then-independent Council member McDuffie resigned to enable him to run for mayor as a Democrat. Under the city’s Home Rule Charter adopted by Congress, that At-Large seat is restricted to a “non-majority party” candidate, meaning a non-Democrat.
The three candidates running for the seat, all independents, include incumbent Doni Crawford, who was temporarily appointed to the seat earlier this year; former D.C. Council member Elisa Silverman; and Jacque Patterson, president of the D.C. Board of Education. All three have expressed support for LGBTQ issues. GLAA issued a +6.5 rating for Crawford and a +5.75 rating for Silverman.
In the race for D.C. Attorney General, Capital Stonewall Democrats has endorsed incumbent Brian Schwalb, who is an outspoken LGBTQ rights supporter. He is being challenged in the Democratic primary by D.C. attorney and law firm partner J.P. Szymkowicz, who is a Ward 3 Advisory Neighborhood Commissioner.
Attorney and local law firm partner Manuel Rivera is running unopposed for the Attorney General office in the Republican primary. No Statehood Green Party candidate is running for the AG post. GLAA issued a rating of +4.5 for Rivera but did not issue ratings for Schwalb or Szymkowicz.
Finally, in the race for the so-called “shadow” D.C. U.S. Senator and D.C. U.S. Representative—offices with no voting or official authority in Congress that were created to lobby Congress on behalf of D.C. issues—Capital Stonewall Democrats did not make an endorsement. In the Democratic primary Paul Strauss is running unopposed for the shadow U.S. Senate seat and Franklin Garcia is running unopposed for the shadow U.S. House seat. Both have been LGBTQ rights supporters.
No Republican or Statehood Green Party candidates are running for either of the two “shadow” positions. GLAA does not issue ratings for the two positions.
Following are short excerpts from the detailed statements four of the seven Democratic mayoral candidates submitted to the Capital Stonewall Democrats or the Washington Blade.
Kenyan McDuffie: “As mayor, every piece of legislation I sign, craft, or endorse should also encompass the interest and input of the LGBTQ community members and advocates…From housing to health care and everything in between… We have a dire crisis regarding the rise in homelessness especially among the youth in our LGBTQ communities. In my administration that simply cannot be the status quo and will not be…I have been a consistent champion for our LGBTQ community and will remain so as mayor of D.C.”
Janeese Lewis George: “As mayor, I will protect our LGBTQ+ neighbors against federal attacks on their identity, including their health care…On the Council I have been a strong supporter of pro-LGBTQ+ bills, including making D.C. a sanctuary for people seeking gender-affirming health care as well as addressing discrimination and harassment in nightlife and hospitality…And as mayor, I am prepared to move up and win those fights – a fight for D.C. statehood, a fight for our true economy, and a real opportunity to uplift our Black queer and trans youth.”
Gary Goodweather: “A Goodweather administration will defend every D.C. law protecting LGBTQ residents. I will establish a Defend DC office to coordinate the District’s legal and public response to federal overreach, with LGBTQ+ protections explicitly within its mandate…My affordable D.C. plan will produce 50,000 new homes with 36,000 affordable units, and I will ensure LGBTQ+ youth housing programs are funded as a budget priority.”
Rini Sampath: “I am an immigrant, proud queer woman, and a 10-year resident of Washington, D.C…For me, LGBTQ+ voters including transgender and nonbinary residents, are not a separate or symbolic constituency; they are a core part of a broader, multiracial, cross-ward coalition rooted in equity and opportunity.”
Vincent Orange: “I have a long and consistent record of supporting LGBTQ+ equality and inclusion in the District of Columbia, grounded in both policy and personal commitment. As the District’s Democratic Committeeman from 2006 to 2015, I publicly supported marriage equality and voted accordingly … During my time on the D.C. Council, I worked to advance protections for LGBTQ+ residents, including authoring and passing legislation to prohibit discrimination against transgender individuals in the workplace.”
15 LGBTQ candidates running for Democratic State Committee
At least 15 known LGBTQ candidates are running for seats on the D.C. Democratic State Committee in the city’s June 16 Democratic primary.
Under local Democratic Party rules, the State Committee includes a total of 38 members, half of whom must be women and half of whom consist of men. The highest two positions include National Committeeman and National Committeewoman. Other positions include seven At-Large Committee men and seven At-Large Committee women, and two Committee men and two Committee women for reach of the city’s eight wards.
Democratic primary voters can vote for as many as seven At-Large male and At-Large female candidates and for two male and two female candidates in each of the ward committee races.
The known LGBTQ Democratic State Committee candidates are as follows:
National Committeeman
Phillip Pannell, Free DC Slate
David Meadows, Democrats United to Free DC slate
At-Large Committeeman
Jordan Kagelmayer, Free DC slate
Malake Glee, Free DC slate
At-Large Committeewoman
Lia Lake Kuduk, Free DC slate
Sonya Joseph, Free DC slate
Ward 1 Committeewoman
Vita Rangel, Free DC slate
Ward 2 Committeeman
Steven M. McCarty, Free DC slate
John Fanning, Democrats United to Free DC
Ward 3 Committeeman
Kurt Vorndran, Democrats United to Free DC slate
Michaell Haresign, Democrats United to Free DC slate
Ward 4 Committeewoman
Corey Welcher
Ward 7 Committeeman
Jimie Williams, Democrats to Free DC slate
Ward 8 Committeeman
Alejaibra Sloan, Free DC slate

Congressional Cemetery hosts Gays & Graves

Baltimore Pride is here

Calendar: June 12-18

Gender-bending buddy film gets 4K restoration for 25th anniversary

German group slams White House’s LGBTQ rights record ahead of World Cup

‘Mighty Real’ explores history of LGBTQ music

D.C.’s housing reality: Cautious optimism meets landlord strain

Hundreds of thousands expected to attend D.C. Pride events

PHOTOS: Pride Run