National
GLAD changes its name
Boston-based LGBT legal advocacy group formed in 1978


GLAD announced its name change in a video posted to YouTube. (Image courtesy YouTube)
BOSTON – A New England-based LGBT legal advocacy group on Feb. 23 announced that it has changed its name.
Gay and Lesbian Advocates and Defenders, which formed in 1978 in response to an anti-gay police sting at the Boston Public Library, is now GLBTQ Legal Advocates and Defenders. The new name ensures that the organization will still be known by the acronym GLAD.
“GLAD has blazed a trail of legal victories for gay, lesbian, bisexual, transgender and queer people across New England and the nation,” said GLAD Executive Director Janson Wu in a press release that announced the name change. “As we continue our pioneering work, we’re proud to bring all of our communities into our name.”
GLAD is the latest LGBT advocacy group to change its name in recent years.
The National Gay and Lesbian Task Force in 2014 announced it had changed its name to the National LGBTQ Task Force. Parents, Families and Friends of Lesbians and Gays in the same year changed its name to PFLAG.





National
Queen Jean is Tony’s first transgender winner
Designer/activist wins for work on ‘Cats: The Jellicle Ball’

It was a historic night at the 79th annual Tony Awards on Sunday as Queen Jean won the award for Best Costume Design of a Musical, making her the first out transgender person to win a Tony.
“This experience has been monumental. We are here for the legacy of queer people, trans people,” she said. “We are taking up space in ways we have to take up space. We have to shift the paradigm. So I just want to say, thank you all so much for this incredible honor. The world right now is deeply, deeply combating so many ailments, and we know as a society that when we come together, we can make real, permanent change.”
She won the award for her work on “Cats: The Jellicle Ball” and was also nominated for best costume design of a play for “Liberation.”
In addition to her stage work, Queen Jean is the founder of Black Trans Liberation, an organization that supports trans and gender-nonconforming people in New York City.
National
Madonna turns Times Square into massive dance floor
Pop icon celebrates Pride month with surprise performance

Pop icon Madonna celebrated Pride month with a pop-up performance in New York City’s Times Square on Thursday to the delight of 50,000 fans.
She performed for about 15 minutes high above street level, including several songs from her new album “Confessions II” due on July 3, along with a trio of songs from the first “Confessions on a Dance Floor.”
In addition to the brand new “Love Sensation,” she performed “I Feel So Free” and “Bring Your Love,” plus “Hung Up,” “Get Together” and “I Love New York.” She wished the crowd a happy Pride season; the event was shared with audiences through Grindr’s first-ever livestream.


National
Gallup finds LGBTQ support among Americans is dropping
Marriage equality support lowest since 2016
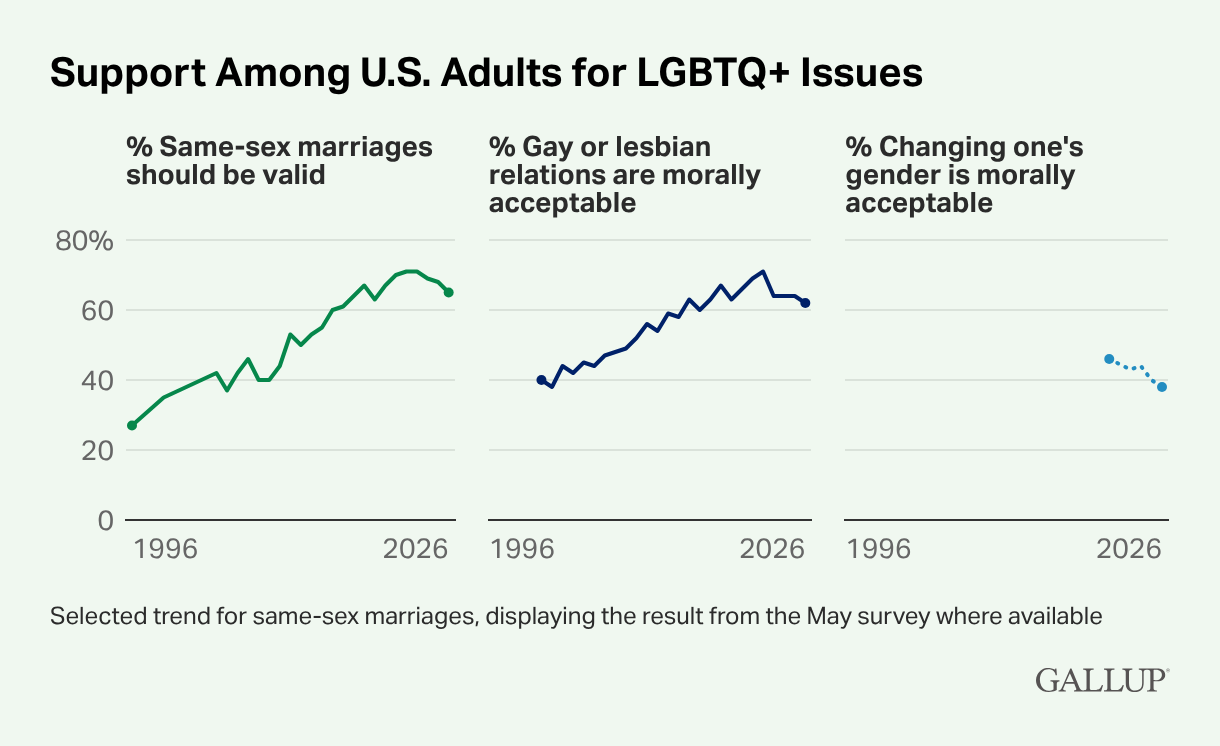
Gallup, one of the leading organizations in public opinion polling, has found that LGBTQ support among Americans is dropping.
The poll, whose data was collected using Gallup’s annual Values and Beliefs survey, was conducted in May and was published on Wednesday. The data was collected through telephone interviews from a sample of more than 1,000 adults living in all 50 states and D.C. using random digit dialing.
It highlights declining attitudes surrounding LGBTQ issues in multiple areas — from support for same-sex marriage to views on gender identity and the morality of one’s sexuality.
One of the most striking findings was that support for marriage equality fell six points from its 2022-2023 high.
The survey also found that 62 percent of Americans view gay and lesbian relations as morally acceptable, the lowest level since 2016 just after same-sex marriage was legalized nationwide by the U.S. Supreme Court.
One newer question on the poll found that the perceived morality of changing one’s gender has dropped eight points since 2021, indicating the American public is less supportive of transgender people.
The data attributes much of the decline to shifting Republican views alongside the party itself. Conservative leaders have pushed back against diversity, equity, and inclusion programs that were intended to foster greater acceptance of LGBTQ people and other historically disadvantaged groups.
President Donald Trump has been a guiding force behind waves of anti-LGBTQ sentiment, particularly when it comes to trans rights. The president has enacted multiple executive orders, including Executive Order 14168, “Defending Women from Gender Ideology Extremism and Restoring Biological Truth to the Federal Government,” which mandates that gender be defined by one’s sex assigned at birth. He also signed Executive Order 14183, “Prioritizing Military Excellence and Readiness,” which barred qualified trans applicants from joining the military and led to the removal of trans service members already serving in the armed forces.
Additionally, he signed Executive Order 14201, “Keeping Men Out of Women’s Sports,” which prohibits trans female athletes from participating on women’s and girls’ sports teams.
In February, Gallup found that an estimated 9 percent of Americans identified as part of the LGBTQ community in some form.
The organization also found that 23 percent of adults under age 30 identify as LGBTQ, compared with 10 percent of those ages 30 to 49 and 3 percent or less among those ages 50 and older.

PHOTOS: Fairfax City Pride

EXCLUSIVE: Pelosi reflects on four decades of LGBTQ advocacy

D.C. prepares to party as Pride celebrations kick off Saturday

David Archuleta, Monroe Alise named D.C. Pride parade marshals