Opinions
PrEP not ready for prime time
Data supporting drug for HIV prevention weak, inconclusive

By JAMES DRISCOLL, Ph.D.
Government picking favorites among technologies on the basis of politics is always risky.
Political favoritism that clears a regulatory path for marketing a new, incompletely tested, drug can cost lives.
Under pressure from Gilead Sciences and its AIDS advocate allies, the FDA antivirals advisory panel will soon consider accelerated approval for Gilead’s AIDS treatment drug Truvada for prevention of HIV infection. Opposition is widespread in the HIV advocacy and medical communities. AIDS advocates warn that such approval would be, at best, years premature. At worst, it would be an unwarranted, dangerous experiment with public health.
Clinical trial data supporting Truvada as prevention, or PrEP (pre-exposure prophylaxis), is weak and inconclusive. PrEP is a far less effective preventative than are condoms (44% versus 98+% in U.S. conditions). Doctors fear that PrEP will be used instead of condoms or that its use will discourage condom usage. Cynthia Davis, an HIV doctor at Drew University of Medicine in Los Angeles, counsels that the drug must show 90 percent efficacy to be used safely in the U.S.
Davis worries that too many people will think that because they are taking the pill they will be safe. Dr. Kevin Fenton, CDC Chief of HIV-AIDS Prevention, has warned: “Some studies suggest that even a small increase in risk behavior due to a false sense of security about the pills’ effectiveness could actually increase HIV infections.”
Drug adherence among those already infected is difficult; it will be even more so among the uninfected. If the uninfected lack therapeutic levels of Truvada in their bloodstream before sex, they will remain unprotected. Patients will need careful monitoring and counseling to insure adherence; such handholding will be costly, inconvenient and in today’s economy unlikely.
Truvada is the most widely used anti-retroviral (ARV). Poor adherence, by the uninfected, will generate drug resistant viral strains. Curbing Truvada resistant strains is important to the well being of the HIV infected population and critical for those who become infected in the future.
ARVs are toxic, healthy people shouldn’t just pop them like vitamin C. The long-term toxicities of Truvada are unknown. Kidney damage, diabetes and hypertension have all been reported. Why risk these toxicities when safer, more effective prevention methods are readily available?
The NIH 052 study has proven that ARV treatment is 96+ percent effective in preventing infection of HIV-negative partners. Indeed, Science named 052’s results the No. 1 scientific advance of 2011.
Resources for ARV treatment in the U.S. are stretched to the limit. PrEP approval will result in scarce resources being diverted from proven preventatives that are 96+ percent effective into an experimental preventive which, even with ideal adherence, promises only 44 percent efficacy.
At $13,000/patient/ year retail, Truvada is a very expensive drug. In an era of severe fiscal constraints, Truvada used as PrEP would not only risk human lives, it would misallocate public and private resources needed for the healthcare of all Americans.
FDA Commissioner Margaret Hamburg has rebuffed appeals to meet with AIDS doctors and advocates who oppose accelerated approval for PrEP. She is ‘too busy’ to listen to them about either the health risks of PrEP or the political influence on its behalf. During the Clinton administration, Commissioner David Kessler met with AIDS advocates more than 20 times to discuss drug approvals.
Kessler’s door was open, he listened. Dr. Hamburg and her staff could learn from Dr. Kessler. One hopes the Obama White House can accelerate her learning curve — she appears to be stalled at go.
The FDA plays a crucial role in the fight against AIDS. When FDA listens to all AIDS advocates, it advances the solutions. If FDA closes the door to all but its friends, it becomes part of the problem.
President Obama has given America its first National AIDS Strategy, increased resources for HIV testing and ADAP, and sustained funding for international AIDS treatment in a difficult fiscal environment.
President Obama has listened and responded. The FDA needs to follow his example.
James Driscoll, Ph.D. is a longtime AIDS activist and an adviser to AIDS Healthcare Foundation.





Opinions
Pride in a new world order
White House has dismantled global U.S. LGBTQ rights infrastructure

It can be tempting to feel somber this Pride. In 2025 and 2026, the United States dismantled much of the LGBTQ+ rights infrastructure it had spent decades building — eliminating the Global Equality Fund, defunding local LGBTQ+ organizations, and banning the rainbow flag from federal buildings and embassies. India unexpectedly rolled back transgender rights in March, stripping away the hard-won right to self-identify. Senegal passed an abhorrent anti-LGBTQ+ law in April, and a similar one just cleared parliament in Ghana.
But this is only part of the story. 2026 is also the year Rob Jetten — a proud gay man — became prime minister of the Netherlands, the youngest in the country’s history. It is the year Thailand celebrated the first anniversary of legalizing same-sex marriage, a historic first for Southeast Asia that is already influencing debates across the region. It is also the year “Heated Rivalry” became one of the most-watched shows on HBO, a global phenomenon.
In fact, LGBTQ+ people have never been more numerous, more visible, or more politically consequential than we are today. The question is not whether we have power. The question is whether we are using it to adapt to the emerging new world order.
Three geopolitical forces are redrawing the terrain. Borders and sovereignty are under renewed strain — this year showed us that the rules-based international order can no longer be taken for granted. Power politics is back at the center of global affairs, and when nations turn inward and militarize, those at the margins often pay the price first. And the institutions our movement has relied on most — governments, multilateral bodies, and multinational corporations — are proving unreliable allies.
The conclusion is that LGBTQ+ people cannot tie their future solely to the fortunes of liberal democracies. We need to come into our own power, and this turbulent moment may offer an opportunity to do so.
This requires a change in strategy. The LGBTQ+ movement has largely understood itself as a national movement in the business of changing hearts and minds one country at a time: win the courts, shift public opinion, and trust that progress would spread from north to south. That model delivered real victories on decriminalization, anti-discrimination protections, military service, and marriage equality. But it is showing diminishing returns. Today, political movements, financial flows, cultural narratives, and AI models increasingly operate globally outside of normative frameworks. Our movement has not kept pace.
LGBTQ+ people globally constitute a population larger than that of the United States. Our collective economic power approaches $4 trillion. We shape culture disproportionately in film, fashion, technology, and the arts. We are no longer a niche constituency petitioning for tolerance. We are a global community with growing economic, cultural, and political influence.
Realizing that potential requires three things. The first is unity — not uniformity, but the strategic coherence that allows a dispersed global community to act with shared purpose. The second is infrastructure: organizations and networks capable of operating across borders, pooling resources, and articulating a vision people want to be a part of. The third is abandoning a Western-centric mindset: building deeper roots in emerging economies will be essential.
There is a broader point. LGBTQ+ people should not be reduced to merely enduring or surviving this moment. We are entering a turbulent period in which humanity faces serious challenges — armed conflict, climate disruption, and technologies advancing faster than governance. LGBTQ+ people have often had to imagine a different future before it existed — and build the communities to sustain it across borders, generations, and class lines. That experience gives us a comparative advantage in this global context.
Pride, at its best, has always been a declaration of existence and a demand for dignity. In 2026, it should become something more: a reckoning with how much power our community has accumulated — and how seriously we intend to wield it to shape what comes next.
Fabrice Houdart is a former World Bank and United Nations staff member. He has taught at Georgetown University and Columbia University, and chairs the Institute of Current World Affairs in D.C.
Opinions
A vice president marches by our side
New exhibit explores Pride in the 2020s and asks what’s to come
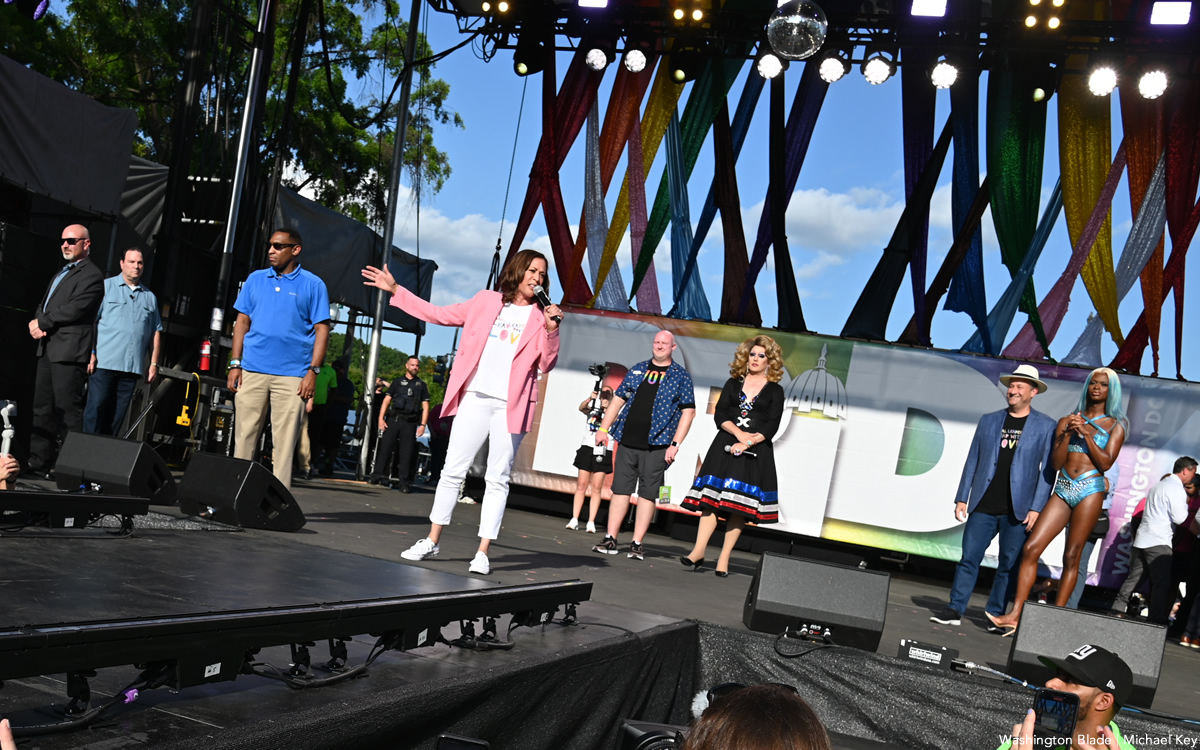
A photograph can change how we understand ourselves. In Rainbow History Project’s exhibit “Pickets, Protests, and Parades: The History of Gay Pride in Washington,” one pairing does exactly that: 10 Washingtonians in their Sunday best picketing the White House in 1965, and, a few panels later, Vice President Kamala Harris in a “Love is Love” Tshirt marching down Pennsylvania Avenue for Capital Pride in 2021. Between those two moments—anxious, buttonedup defiance on one side of the White House fence and a sitting vice president cheering among rainbow flags on the other—lies the story this exhibit tells.
Last year, we stretched that story along Freedom Plaza for WorldPride 2025, just three blocks from the White House. Over seven weeks, visitors from around the globe walked a timeline that showed how a small, risky White House picket helped ignite six decades of increasingly visible, intersectional Pride in the nation’s capital. They met organizers who insisted that gay history did not start at Stonewall, and that D.C. has been a laboratory for LGBTQ resistance since at least that first 1965 picket.
This June, as part of Dupont Underground’s “Matters of Pride” programming, we’re inviting you back underground to revisit what we showed the world last year—and to look harder at what it asks of us now. The tunnels below Dupont Circle will host the early eras of the exhibition: the White House picket; block parties at Lambda Rising bookstore, the first National March for Lesbian and Gay Rights in 1979 that brought more than 100,000 people onto the Mall; and the first D.C. Pride march that began at Howard University, led by BIPOC activists who carried every part of their identities into the streets.
Seen together, these moments make the theme “A Vice President Marches By Our Side” less about a single VIP participant and more about a changing relationship between our movements and the state. In 1965, picketers carefully followed dress codes to appear “employable” enough to be heard at all. By 1979, marchers filled the National Mall with banners that linked sexuality to feminism, racial justice, and antiwar activism. By the 2020s, a vice president could show up at Capital Pride, call for the Equality Act, and speak explicitly about protecting trans youth and communities of color. None of those shifts were guaranteed. All of them were built, step by step, by people who kept organizing whether or not anyone in power joined them.
The reinstall is also a chance to notice details you may have rushed past on a crowded WorldPride weekend: a handlettered sign demanding federal jobs in 1965; a quote from a 1970s organizer about the sheer relief of dancing in public; a photograph of local pioneers like SaVanna Wanzer, the founder of D.C. Trans Pride and Black Trans Pride, whose work helped make today’s Pride more fully trans inclusive even as Black trans folx remain under attack. These are not just artifacts; they are reminders of how much was risked so that we could take Pride for granted at all.
We are reinstalling this exhibit at a moment when very little about the future feels guaranteed. America’s 250th birthday is around the corner, and national debates over whose stories “belong” in the classroom, the public square, or in the archives, are already shaping policy. In that context, going back to the origins of D.C. Pride is more than nostalgia. It is a strategy lesson. The 1960s picketers, the 1979 marchers, the BIPOC activists leaving an intersectionality conference at Howard and marching to the Mall—all of them faced hostile climates, limited resources, and no certainty of success. Yet they showed up anyway, and in doing so, they expanded what was imaginable.
That is why, at the end of the reinstall, the exhibit turns back on you. The final section, “The Next 60 Years of Pride,” remains intentionally unwritten. Instead, you will find a simple question on the wall: “What will you do?” Visitors will have the chance to add their own commitments—large or small—to the story: what they will march for, organize for, or quietly sustain in the years ahead.
A vice president once marched by our side. This month at Dupont Underground, we are asking something both humbler and more radical: after everything we have learned from the past six decades of Pride in Washington, who will you be standing with, and what will you be brave enough to do next?
In conjunction with WorldPride 2025 the Rainbow History Project exhibited “Pickets, Protests, and Parades: The History of Gay Pride in Washington.” More than two years of planning resulted in seven weeks of outdoor education, centering the voices of Pride’s organizers. In the final of the 10 themes, we discuss “A Vice President Marches By Our Side,” about what Pride looked like in the 2020s and asking about Pride in the years to come.
Vincent Slatt volunteers as the senior curator at the Rainbow History Project.
Opinions
Leaving for a barge trip through canals of Burgundy
Nervous about European reactions to Americans given Trump’s war in Iran

As those who read my columns know, I love cruising, the kind you do on water. I have had many different cruise experiences, including sailing through the Galapagos and the Norwegian fjords. This time, I will be doing something a little different and am off on a new adventure. With 18 others, will be on a barge for six days, going from Lyon to Paris, through the canals of Burgundy. Each day will bring a new adventure. We will be embarking in Besancon, and traveling to Beaune, Arc-et-Senans, Dole, Saint-Jean-De-Losne, Seurre, Chalon-Sur-Saone, and then disembarking in Auxerre, en route to Paris. Of the 18 people, four are friends from D.C. and Rehoboth Beach. I look forward to meeting the other travelers.
I leave for Paris on June 8 and made arrangements for a car in Paris to take me to the Gare De Lyon, to board a fast train to Lyon. A quick two-hour trip. In Lyon I will head to the hotel for a welcome dinner, where I will meet our guide and other travelers. This is a Gate 1 adventure booked by my friends at My Lux Cruise. We will be spending two days in Lyon before boarding the MS Daniele, built in 2016. It is modern, with space for both indoor and outdoor dining, a small lounge, the requisite bar, and very simple staterooms. Mine will have two single beds. Can’t forget the hot tub on the bow. I will be writing a blog during my trip, which will be published in the Blade, likely after my return. I will post pictures during the trip on social media. After six days on the barge, we arrive in Paris, where I will spend a couple of days with good friends. One planned excursion is to see the rebuilt Notre Dame.
I will be away from D.C. on June 16, primary day. Since for the first time there will be ranked choice voting, it is possible we won’t know who wins until I get back on June 19. I hope everyone votes, and urge you to vote, as I already have, for Kenyan McDuffie for mayor. His main opponent, Janeese Lewis George, clearly doesn’t understand how D.C. government really works. She is trying to emulate NYC Mayor Mamdani with promises, but hers won’t happen. We don’t have a governor, and state legislature, to help. Our governor is in essence the felon in the White House, and our state legislature is the Congress. They won’t be helping. In addition, George has claimed the endorsement of an antisemitic organization, DSA, and is going to birthday parties for a guy who calls gay men like me ‘fags’ and says they shouldn’t be teaching his children in the public schools. The winners of the Democratic primary races will determine how D.C. moves forward. It really makes a difference.
The world is a different place today than it was just a short 18 months ago, when the felon began his second term. This is the first time I will be out of the country since he began this illegal war with Iran, plunging the world into chaos. I wonder what the reception for an American will be in Europe these days. I remember back when Ronald Reagan was first elected, which was the last time in my travels, before Trump, I felt compelled to apologize for my country. At that time people would actually come up to me and ask, what did America do, and why? Yet as bad as times seemed then, they were nowhere as bad as they are today. The felon in the White House has made life so much worse for people around the world. Europeans have seen him get on his knees to Putin, and screw Ukraine. Now with this illegal, and unnecessary, war in Iran, he is impacting their lives directly. Fuel prices are rising dramatically, and there is a drastic shortage of jet fuel, causing cuts in flights. They see him work hand-in-hand with the war criminal, Netanyahu, in Israel. They see how he simply wants to enrich himself with things like his ‘Board of Peace,’ and in the long run, screw the Palestinian people. It will be interesting to hear how Europeans feel about all this. I look forward to listening to them. All I can say in response is I didn’t vote for Trump and will continue to demonstrate, and write against him, as often as I can.
Putting politics aside, which is hard to do these days, I am excited about this new adventure, and look forward to sharing some of my experiences with you.
Peter Rosenstein is a longtime LGBTQ rights and Democratic Party activist.

Blade editor inducted into D.C. Society of Professional Journalists Hall of Fame

Pride in a new world order

McDuffie on LGBTQ support and standing up to Trump

PHOTOS: Fairfax City Pride